
FOI 24/25-1472
to be permanent. The impairment is, or is likely to be permanent only if the impairment
does not require further medical treatment or review in order for its permanency or likely
permanency to be demonstrated (even though the impairment may continue to be treated
and reviewed after this has been demonstrated)”. This is slightly different to Section 5.4 in
that if further treatment is recommended, you may not be able to determine the
permanency of the impairment, this would therefore mean Section 24(1)(b) is not met. You
do not need to know the outcomes for this treatment. The important part of this section
though is the last sentence – the impairment can stil be treated and reviewed after
permanency has been demonstrated. A good example of this are psychosocial disabilities.
People wil quite often engage in maintenance treatment, not to remedy the impairment but
to maintain it and prevent it from declining. If the evidence demonstrates the impairment is
permanent but they stil require treatment for maintenance then Section 24(1)(b) would be
met. If it is not referred to in the evidence, it is important to clarify whether the listed
treatment is to remedy the impairment or for maintenance.
**CLICK FOR NEXT PARAGRAPH**
The final section is section 5.7 which states “if an impairment is of a degenerative nature,
the impairment is, or is likely to be, permanent if medical or other treatment would not, or
would be unlikely to, improve the condition”. This means that if the impairment is
degenerative in nature then it is likely permanent. When assessing the evidence you need to
determine that the impairment is degenerative and not the condition. Refer back to the
points in the technical meeting for Section 24(1)(a) for a refresher on determining what the
impairment is.
**CLICK FOR NEXT SLIDE**
Page 300 of 362
FOI 24/25-1472
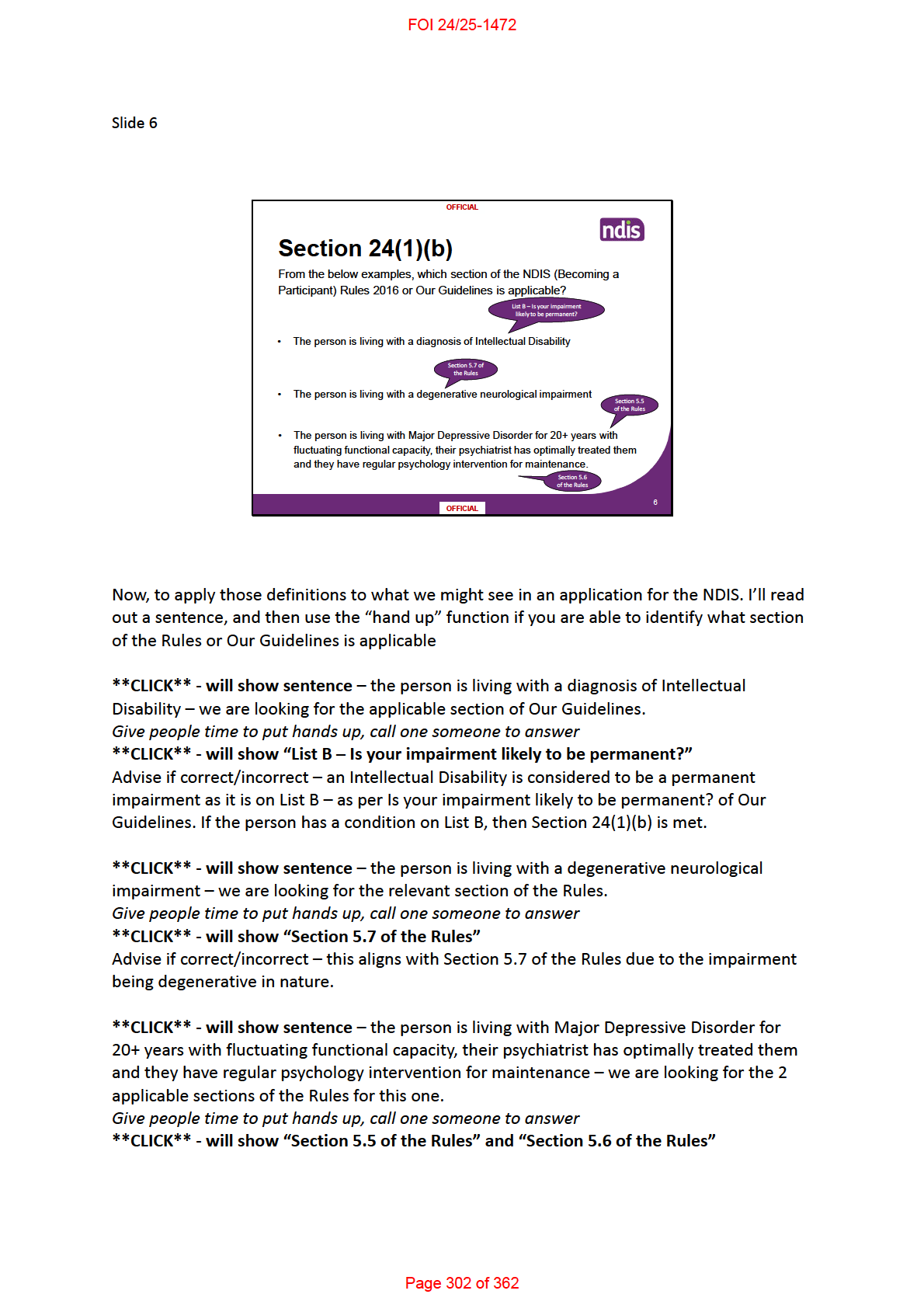
Advise if correct/incorrect – this has 2 applicable sections of the Rules – 5.5 due to the
fluctuating nature of the impairment, and section 5.6 as the impairment continues to be
treated after permanency has been established.
Page 303 of 362
FOI 24/25-1472
Page 307 of 362
FOI 24/25-1472
reduction. If the EOD was indicating she does have a substantial reduction then it would be
recommended to seek further information on permanency.
**CLICK FOR NEXT SLIDE**
Page 310 of 362
FOI 24/25-1472
**CLICK FOR NEXT SLIDE**
Page 313 of 362
FOI 24/25-1472
If the treatment is likely to remedy the impairment then Section 24(1)(b) would not be met
in line with Section 5.4 of the NDIS (Becoming a Participant) Rules 2016.
**CLICK FOR NEXT PAGE**
Page 315 of 362
FOI 24/25-1472
The answer is false
– It is important to remember that permanency must be demonstrated
and not just stated. There is no other information on treatment options and therefore
permanency cannot be determined. If this was someone older who has an established
diagnosis of Schizophrenia, as the delegate you could determine that Section 24(1)(b) is met
as the impairment could be considered likely to be permanent. However for a young person,
more information is required than a sentence stating the impairment is permanent.
**CLICK FOR NEXT PAGE**
Page 317 of 362
FOI 24/25-1472
•
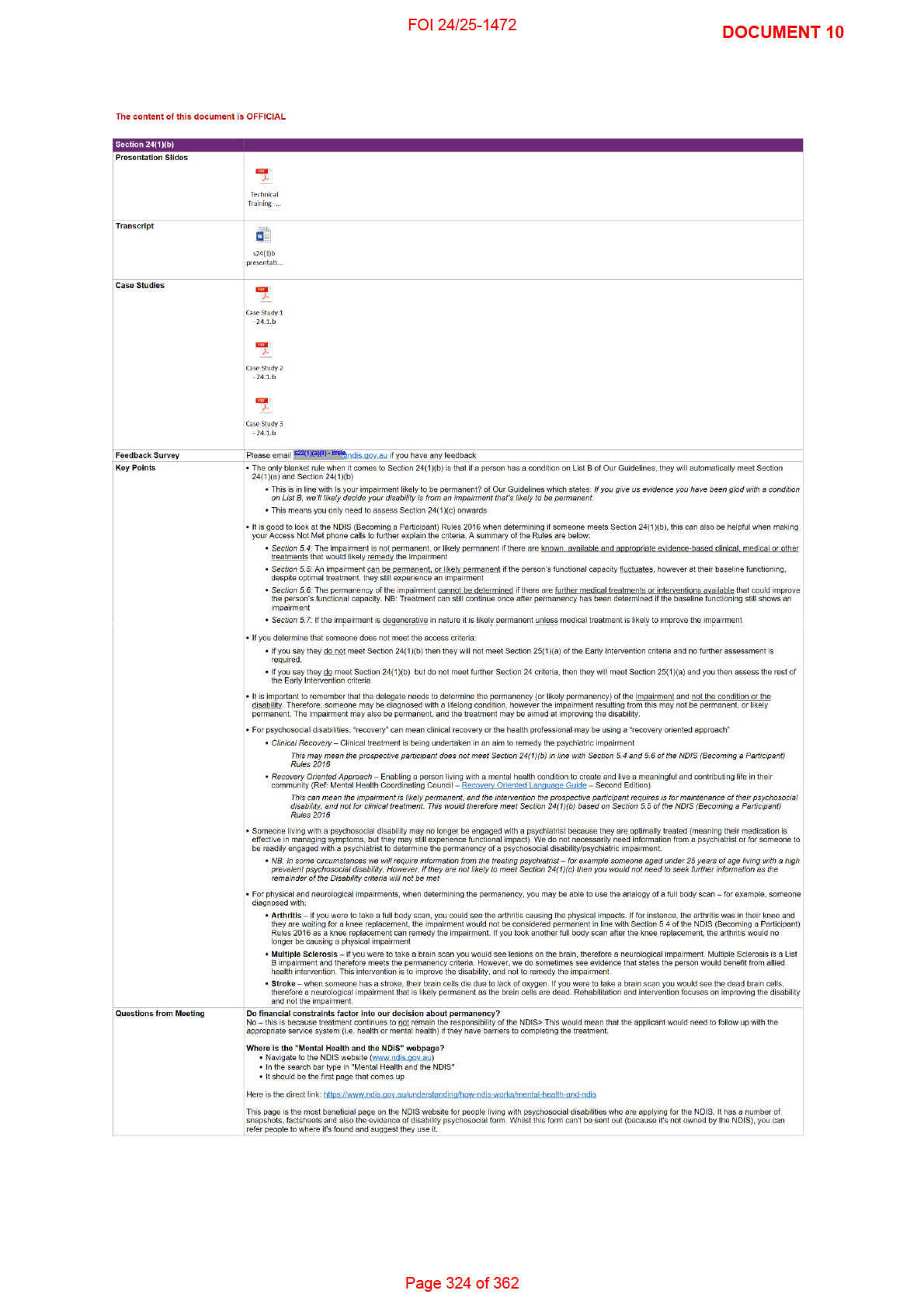
Section 5.7: If the impairment is degenerative in nature it is likely permanent
unless medical treatment is likely to improve the condition.
**CLICK FOR NEXT SLIDE**
Page 319 of 362
FOI 24/25-1472
•
Recovery Oriented Approach – Enabling a person living with a mental health condition to
create and live a meaningful and contributing life in their community (Ref: Mental Health
Coordinating Council – Recovery Oriented Language Guide – Second Edition)
This can mean the impairment is likely permanent, and the intervention the
applicant requires is for maintenance of their psychosocial disability, and not
for clinical treatment. This would therefore meet Section 24(1)(b) based on
Section 5.5 of the NDIS (Becoming a Participant) Rules 2016
**CLICK FOR NEXT SLIDE**
Page 321 of 362
FOI 24/25-1472
**CLICK FOR PARAGRAPH**
Stroke – when someone has a stroke, their brain cells die due to lack of oxygen. If you were to take a
brain scan you would see the dead brain cells, therefore a neurological impairment that is likely
permanent as the brain cel s are dead. Rehabilitation and intervention focuses on improving the
disability and not the impairment.
**CLICK FOR NEXT SLIDE**
Page 323 of 362
FOI 24/25-1472
*Click* [to go to next slide]
Page 328 of 362
3
FOI 24/25-1472
impairment.
An example of this is the impairment of a Stroke. When someone has a stroke, their brain cells die due to lack of
oxygen. If you were to take a brain scan you would see the dead brain cells, therefore a neurological impairment
that is likely permanent as the dead brain cells are a “loss of, or damage to, a mental function”. Rehabilitation
and intervention focuses on improving the disability and not the impairment.
*Click* [to go to next slide]
Page 332 of 362
6
FOI 24/25-1472
*Pause*
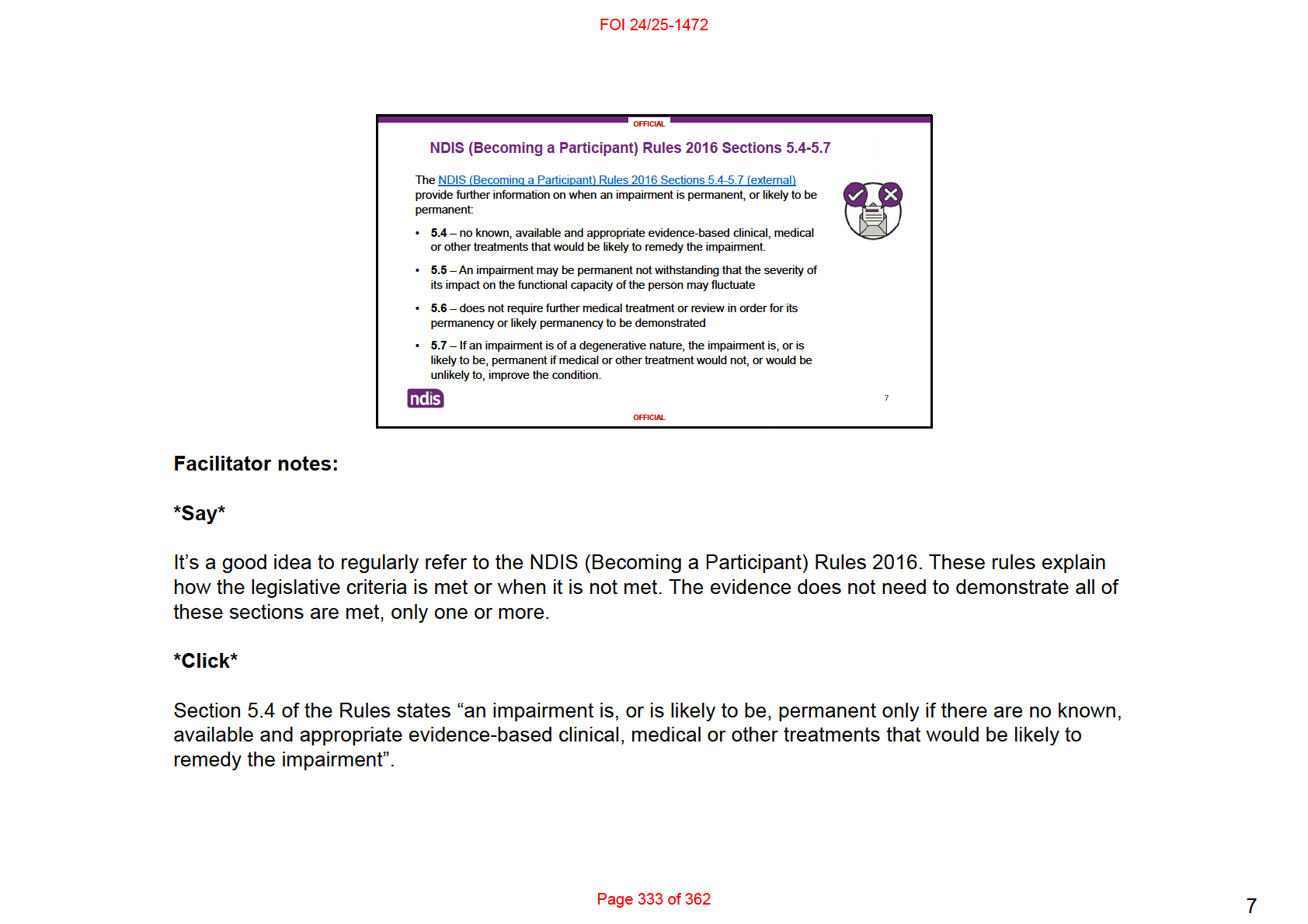
This means that we consider whether the impairment is likely to be permanent after all available and appropriate
treatment options have been pursued.
In some situations, it may be clear an impairment is likely to be permanent while an applicant is still undergoing
treatment or rehabilitation. For example, they may still need treatment and rehabilitation for a spinal cord injury,
but it’s clear they’ll have a permanent impairment.
*Click*
Section 5.5 of the Rules states “an impairment may be permanent not withstanding that the severity of its impact
on the functional capacity of the person may fluctuate or there are prospects that the severity of the impact of the
impairment on the person’s functional capacity, including their psychosocial functioning, may improve”.
*Pause*
An impairment that is episodic or fluctuates in intensity can still be considered permanent due to the overall
impact on the person’s life and the likelihood that they will be impacted across their lifetime. This means that an
applicant might still have a permanent impairment, even if its effects may change over time.
*Click*
Section 5.6 of the Rules states “an impairment may require medical treatment and review before a determination
can be made about whether the impairment is permanent or likely to be permanent. The impairment is, or is
likely to be permanent only if the impairment does not require further medical treatment or review in order for its
permanency or likely permanency to be demonstrated (even though the impairment may continue to be treated
and reviewed after this has been demonstrated)”.
*Pause*
Page 334 of 362
7
FOI 24/25-1472
This is slightly different to Section 6.4 in that if further treatment or review is recommended, you may not be able
to determine the permanency of the impairment at that point in time.
It is important to note here that a person can still be treated and reviewed after permanency has been
demonstrated.
Psychosocial disabilities are a good example of this. People may engage in maintenance treatment, not to
remedy the impairment but to maintain their functioning and prevent it from declining. If the evidence
demonstrates the impairment is permanent but they still require treatment for maintenance, then Section 24(1)(b)
can be met. If it is not referred to in the evidence, it is important to clarify whether the listed treatment is to
remedy the impairment or for maintenance.
*Click*
The final section is section 5.7 which states “if an impairment is of a degenerative nature, the impairment is, or is
likely to be, permanent if medical or other treatment would not, or would be unlikely to, improve the condition”.
*Pause*
This means that for degenerative impairments, or those that get worse over time, we consider them permanent if
treatment isn’t likely to help or improve the impairment’s effects.
When assessing the evidence, we need to determine that the impairment is degenerative and not the condition.
*Click* [to go to next slide]
Page 335 of 362
7
FOI 24/25-1472
•
The person is living with Schizoaffective Disorder for 20+ years with fluctuating functional capacity, their
psychiatrist has optimally treated them, they have monthly anti-psychotic medication (depot injection) and
regular psychology intervention for maintenance.
[
After 10 minutes bring the group back together to answer the questions]
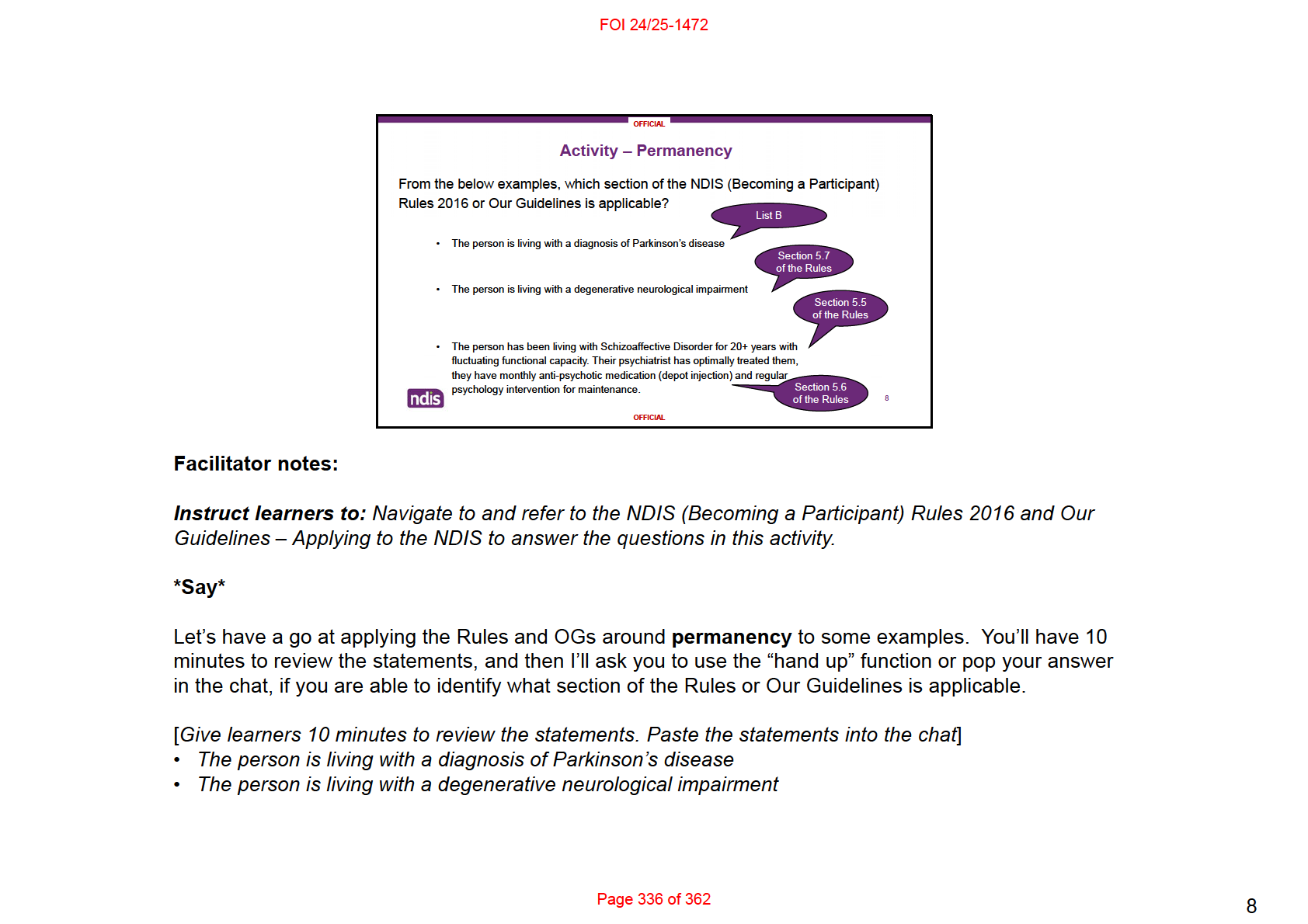
*Click* [
to show sentence] – the person is living with a diagnosis of Parkinson’s disease – we are looking for the
applicable section of Our Guidelines.
*Pause* [
Give people time to put hands up, call one someone to answer]
*Click* [
to show “List B – Is your impairment likely to be permanent?”]
Advise if correct/incorrect – Parkinson’s disease is considered a permanent impairment as it is on List B – as per
Is your impairment likely to be permanent? of Our Guidelines. If the person has a condition on List B, then
Section 24(1)(b) is likely met.
*Click* [
to show sentence] – the person is living with a degenerative neurological impairment – we are looking
for the relevant section of the Rules.
*Pause* [
Give people time to put hands up, call one someone to answer]
*Click* [
to show “Section 5.7 of the Rules”]
Advise if correct/incorrect – this aligns with Section 5.7 of the Rules due to the impairment being degenerative in
nature.
*Click* [
to show sentence] – the person is living with The person is living with Schizoaffective Disorder for 20+
years with fluctuating functional capacity, their psychiatrist has optimally treated them, they have monthly anti-
psychotic medication (depot injection) and regular psychology intervention for maintenance.
– we are looking for the 2 applicable sections of the Rules for this one.
*Pause* [
Give people time to put hands up, call one someone to answer]
Page 337 of 362
8
FOI 24/25-1472
*Click* [
to show “Section 5.5 of the Rules” and “Section 5.6 of the Rules”]
Advise if correct/incorrect – this has 2 applicable sections of the Rules – 5.5 due to the fluctuating nature of the
impairment, and section 5.6 as the impairment continues to be treated after permanency has been established.
*Click* [to go to next slide]
Page 338 of 362
8
FOI 24/25-1472
The reason we are discussing the recovery orientated approach for Psychosocial Disabilities today is because
the word ‘recovery’ can have different meanings, and impact upon how we assess Section 24(1)(b).
For psychosocial disabilities, “recovery” can mean clinical recovery, or it can also mean the health professional
may be using a “recovery-oriented approach”.
• Clinical Recovery may mean that Clinical treatment is being undertaken in an aim to remedy the psychiatric
impairment.
• This may mean the applicant does not meet Section 24(1)(b)
• If a health professional is taking a Recovery Oriented Approach – they may use language to support Enabling
a person living with a mental health condition to create and live a meaningful and contributing life in their
community.
The person is likely to be receiving ongoing treatment, and it is important to review the evidence to determine if
the ongoing treatment is likely to remedy the impairment, or if it is ongoing maintenance treatment. If the
treatment is for maintenance and not clinical in nature, this means the impairment is likely permanent.
This would therefore meet Section 24(1)(b) based on Section 5.5 of the NDIS (Becoming a Participant) Rules
2016.
*Click* [to go to next slide]
Page 340 of 362
9
FOI 24/25-1472
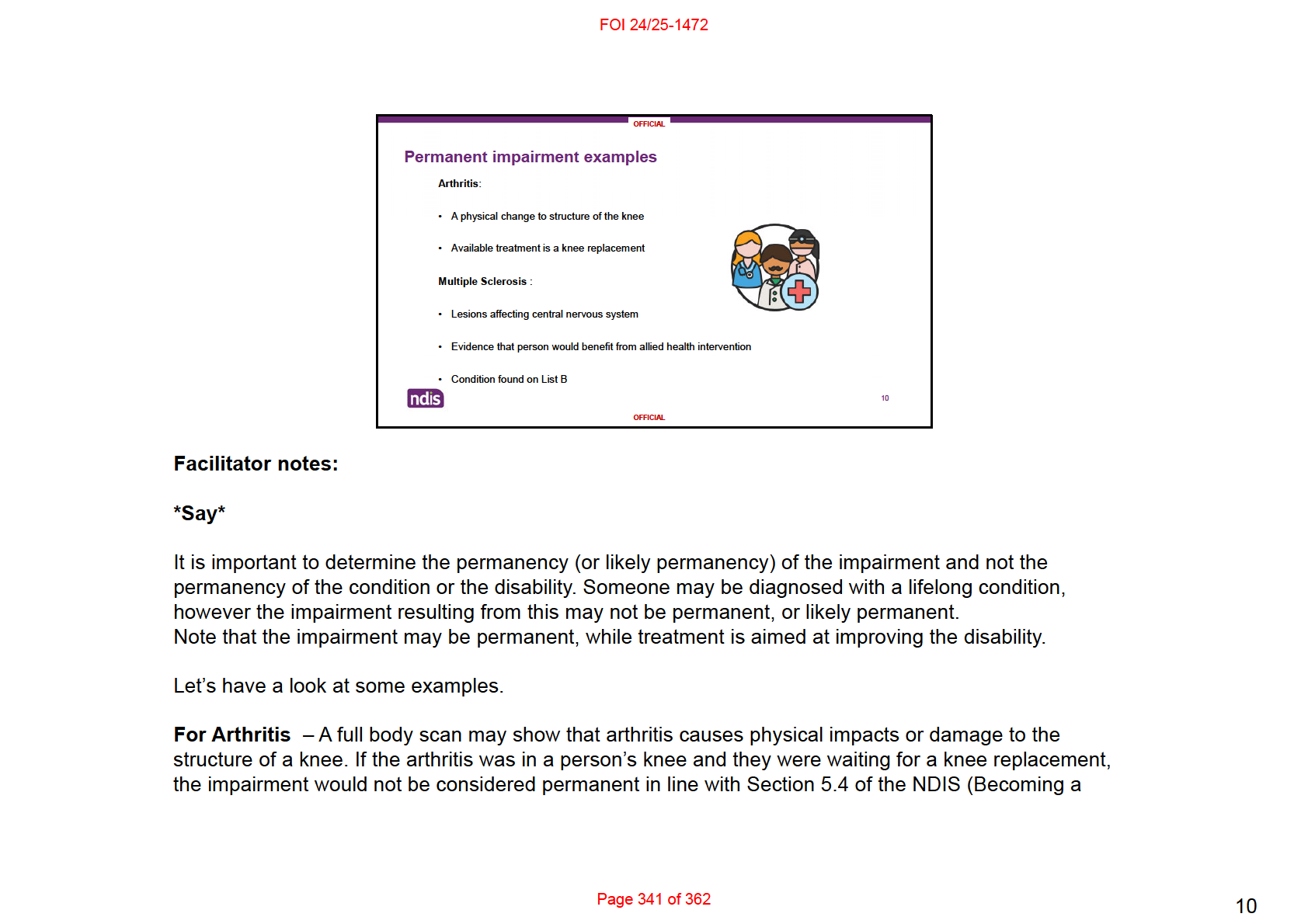
Participant) Rules. This is because a knee replacement could remedy the impairment. If you took another full
body scan after the knee replacement, the arthritis would no longer be causing a physical impairment.
For Multiple Sclerosis – A brain scan would show lesions on the brain and in the nervous system. MS is a
neurological impairment as it causes damage to the central nervous system. Sometimes evidence may also
state the person would benefit from allied health intervention. In these cases, it is likely that this intervention is to
improve the disability, and not to remedy the impairment. Multiple Sclerosis is a List B impairment and therefore
is likely to meet the permanency criteria.
*Click* [to go to next slide]
Page 342 of 362
10
FOI 24/25-1472
permanent in line with Sections 5.4-5.7 of the NDIS (Becoming a Participant) Rules 2016.
*Click* [
to show question]
A person can meet the permanency criteria but continue treatment.
*Click* [
to show answer]
The answer is true – As per Section 5.6 of the NDIS (Becoming a Participant) Rules 2016, the impairment can
continue to be treated after permanency has been demonstrated. If the treatment is likely to remedy the
impairment, then Section 24(1)(b) would
not be met in line with Section 5.4 of the NDIS (Becoming a Participant)
Rules 2016.
*Click* [to go to next slide]
Page 344 of 362
11
FOI 24/25-1472
we have before us.
Okay, next question
*Click* [
to show question]
I’m assessing an application for an 18-year-old with Schizophrenia. Their psychologist states that the
impairments are permanent. I don’t have any other treatment information so will determine that Section 24(1)(b)
is met.
*Click* [
to show answer]
The answer is false
– Permanency must be demonstrated and not just stated. There is no other information on
treatment options and therefore permanency cannot be determined. More information is required.
*Click* [to go to next slide]
Page 346 of 362
12
FOI 24/25-1472
financial constraints.
I’ll now provide you with 15 minutes to review the evidence and answer some questions. I will paste the case
study and the questions into the chat.
Does anyone have any questions before we begin?
*Paste the below questions in the chat*
Q: Does Josephine meet Section 24(1)(a) and (b)? If so, why?
Q: After assessing Section 24(1)(a) and (b), what criteria will you assess next?
*
Answers on next slide
*Click* [to go to next slide]
Page 349 of 362
14
FOI 24/25-1472
(b) are met.
*Click* [
to show question]
After assessing Section 24(1)(a) and (b), what criteria will you assess next?
*Click* [
to show answer]
Correct/Incorrect - You will assess Section 24(1)(c) next. The Access Decision Tree is a tool that can support
you with your decision making, and provide guidance on which criteria to consider next.
*Click* [to go to next slide]
Page 351 of 362
15
FOI 24/25-1472
*Paste the below questions in the chat*
1. Does Annabel have a permanent, or likely permanent, impairment?
2. What section/s of the NDIS (Becoming a Participant) Rules 2016 are applicable?
3. Should you seek further information?
*
Answers on next slide
*Click* [to go to next slide]
Page 353 of 362
16
FOI 24/25-1472
*Click* [
to show question]
What section/s of the NDIS (Becoming a Participant) Rules 2016 are applicable?
*Click* [
to show answer]
Section 5.4 and 5.6 – Section 5.4 and 5.6. There are available and appropriate evidence-based treatments that
Annabel could engage in. For example: pain management clinic, multi-disciplinary team intervention, specialist
intervention, graded exercise and pacing program. These could potentially remedy the impairment (5.4), or as
we do not know the outcome of these treatments, the permanency of the impairment cannot be determined (5.6).
*Click* [
to show question]
Should you seek further information?
*Click* [
to show answer]
No. As Annabel would not meet Section 24(1)(c) further information is not required. Even if permanency could be
established, she does not have a substantial reduction. If the EOD indicated she had a substantial reduction,
then you might seek further information on permanency.
*Click* [to go to next slide]
Page 355 of 362
17
FOI 24/25-1472
I’ll now provide you with 15 minutes to review the evidence and answer some questions. I will paste the case
study and the questions into the chat.
Does anyone have any questions before we begin?
*Paste the below questions in the chat*
1. Does Jamie have a permanent, or likely permanent, impairment?
2. Should you seek further information?
*
Answers on next slide
*Click* [to go to next slide]
Page 357 of 362
18
FOI 24/25-1472
Disorder, the evidence does not indicate if any further treatments for these impairments are being recommended
and what their expected outcomes might be.
*Click* [
to show question]
Should you seek further information?
*Click* [
to show answer]
Correct/Incorrect - No – given the limited information on the treatments undertaken, the recommendation for
further treatment, and the evidence indicating that the PTSD was diagnosed 2 months prior, it would be most
appropriate to make an Access Not Met decision. This is because it is unlikely that the applicant will meet
Section 24(1)(b), and we do not want to prolong an outcome for the applicant.
A beneficial resource to refer to is the “Mental Health and NDIS” page on the external NDIS website. Here you’ll
find different resources and information on people living with a psychosocial disability who are aged under 25
years old.
*Click* [to go to next slide]
Page 359 of 362
19