DOCUMENT 1
FOI 24/25-1836
Fetal Alcohol Spectrum Disorder and Fetal Alcohol Syndrome
The content of this document is OFFICIAL
Fetal Alcohol Spectrum Disorder (FASD) and Fetal Alcohol Syndrome (FAS) can both be
accepted as List B conditions.
The diagnostic guide for Fetal Alcohol Spectrum Disorder (FASD) was updated in Australia in
early 2020, with FASD now diagnosed as a spectrum disorder. A subsequent 2021 Senate
Inquiry Report provided the following description for FASD and FAS:
'FASD encompasses a spectrum of disorders that can arise from alcohol exposure in utero. The
spectrum covers physical, neural, behavioural, and learning difficulties from mild through to
severe symptoms.
‘Perhaps the most clinically recognisable manifestation of FASD is Fetal Alcohol Syndrome
(FAS), which is characterised by physical abnormalities including of the face. In individuals with
FAS, there has usually been exposure to alcohol during the first trimester of pregnancy, when
the face and other bodily organs are forming.'
s22(1)(a)(ii) - irrelevant material
Fetal Alcohol Spectrum Disorder Disability Snapshot
Page 1 of 65
FOI 24/25-1836
DOCUMENT 2
List A - Guidance
The content of this document is OFFICIAL
Intellectual Disability/Intellectual Developmental Disorder
The evidence of disability states one or more of the below:
•
States current DSM as Moderate, Severe or Profound
•
Uses the DSM Code that equates to Moderate, Severe or Profound:
o
318.0 or F71 = Moderate
o
318.1 or F72 = Severe
o
318.2 or F73 = Profound
•
Not sufficient for the evidence to list "Mild to Moderate"
•
Has to be from a listed health professional (multidisciplinary team, paediatrician,
psychiatrist or clinical psychologist, neuropsychologist, educational psychologist or
developmental psychologist)
•
Ensure that the health professional is registered on AHPRA from one of the
above. This may be different to what their signature says.
s22(1)(a)(ii) - irrelevant material
•
It is not sufficient to use the DSM code of 299.00 as this applies to the diagnosis of
Autism, not the severity level
•
Does not need to state DSM-V – this is because the DSM-V is the only diagnostic tool for
Autism that uses Level 2 and 3 is the DSM-V
s22(1)(a)(ii) - irrelevant material
Page 2 of 65
FOI 24/25-1836
s22(1)(a)(ii) - irrelevant material
•
Has to be from a listed health professional (multidisciplinary team, paediatrician,
psychiatrist of clinical psychologist, neuropsychologist, forensic psychologist)
o
Ensure that the health professional is registered on AHPRA from one of the
above. This may be different to what their signature says.
To see more practice guidance on Autism (including List A requirements), refer to Autism.
s22(1)(a)(ii) - irrelevant material
Page 3 of 65
FOI 24/25-1836
s22(1)(a)(ii) - irrelevant material
Registrars and Fellows
If you have evidence from a Registrar or a Fellow (such as a Paediatric Registrar or a Psychiatry
Registrar or paediatric fellow) then this is not sufficient to meet List A unless it has also been
signed off by one of the treating health professionals for List A. This is because when someone
is a registrar/fellow they are still in training for their speciality. We can still accept the diagnosis
as they already hold a medical qualification, however are just not finished their speciality
training. You will also notice that they will not be registered in AHPRA as the specialist.
Therefore the easiest way to determine if they are suitably qualified is to check their
qualifications and specialities on AHPRA.
Page 4 of 65
FOI 24/25-1836
DOCUMENT 3
Intellectual Impairment/Disability/Developmental Disorder
The content of this document is OFFICIAL
Intellectual Developmental Disorder/Intellectual Disability
s22(1)(a)(ii) - irrelevant material
Intellectual Impairment and Intellectual Disability
A diagnosis of Intellectual Impairment and Intellectual Disability should not be used
interchangeably. When diagnosing an Intellectual Disability, both Intellectual Functioning (FSIQ)
and Adaptive Functioning are assessed. Someone can have an intellectual impairment and not
meet the criteria for an Intellectual Disability. Further information on diagnosing an Intellectual
Disability can be found on the American Psychiatric Association website. Although this is an
American website, they are also the developers of the DSM-5.
s22(1)(a)(ii) - irrelevant material
Page 5 of 65
FOI 24/25-1836
s22(1)(a)(ii) - irrelevant material
List A
The evidence of disability states one or more of the below:
•
States current DSM as Moderate, Severe or Profound
•
Uses the DSM Code that equates to Moderate, Severe or Profound:
•
318.0 or F71 = Moderate
•
318.1 or F72 = Severe
•
318.2 or F73 = Profound
Page 6 of 65
FOI 24/25-1836
DOCUMENT 4
Developmental Delay
The content of this document is OFFICIAL
This page contains the following guidance on Developmental Delay:
•
What is Developmental Delay?
•
Developmental Concerns
•
The role of Early Childhood Partners
•
Providing evidence for developmental delay
•
Multiple Sources of Information
•
Making an Access Not Met decision
•
Requesting Further Information
•
Children turning 6 within 90 days
•
Providing feedback after a Request for Further Information
•
Responding to direct outreach from Early Childhood Partners
•
Chronological Age
•
Developmental Milestones
•
Our Guidelines
•
Helpful resources
s22(1)(a)(ii) - irrelevant material
Page 7 of 65
s22(1)(a)(ii) - irrelevant material
FOI 24/25-1836
s22(1)(a)(ii) - irrelevant material
PEDI-CAT
This is a functional capacity
The early
Review scores which will be
In the child’s Pedi-CAT
(Paediatric
assessment. It’s used to help with
childhood
divided into Scaled Scores, T
Person
frequently
Evaluation of understanding a child’s ability to
partner will
Scores and Age Percentiles.
Account >
asked
Disability
complete tasks in their daily life. The 4 facilitate the
Functional
questions |
Inventory
domains of tasks are:
gathering of
T Scores:
Capacity
NDIS
Computer
information
•
below 30 = Assessment
•
Adaptive Test)
Daily Activities from the
Record
decreased case > Case assessment –
•
Mobility
family using
functional
Activity >
the PEDI-CAT.
PEDI-CAT
ability
Assessments.
•
Social/Cognitiv The answers
compared
Frequently
e
to the
to what is
Asked
•
Responsibility. questions will
typically
Questions
be entered
expected
This can assist in assessing the impact into an
for that age
a child’s developmental delay has on external
range
their daily activities.
Pearson site
which will
•
30-70 =
automatically
considered
populate a
within the
score based
expected
on the
range for
answers.
age
The family
•
Above 70 =
may also
above what
provide an
is typically
existing PEDI-
excepted
CAT
for that age
completed
range.
outside of
Age Percentiles:
Pearson, for
example from
•
<5 = below
their child’s
average
doctor. If it is
•
5-24 = low
from within
average
the last 3
months, the
The Responsibility Domain will be
early
0 for children younger than 3 years,
childhood
Page 10 of 65
FOI 24/25-1836
partner will
because scores are not completed
enter this
in this domain for this age range.
score into
PACE. If it is
Please note: The PEDI-CAT is not
from
more
to be used as the only source of
than 3
information used to understand
months ago, the needs of a child. Rather it is
the early
used to contribute to other
childhood
information gathered.
partner
must complete a
new one.
s22(1)(a)(ii) - irrelevant material
s22(1)(a)(ii) - irrelevant material
Page 11 of 65
s22(1)(a)(ii) - irrelevant material
FOI 24/25-1836
s22(1)(a)(ii) - irrelevant material
Developmental Milestones
Developmental Milestones can be used as an information tool to look for patterns of development and behaviour that may suggest that a child is or
is not developing as expected. It is important not to use the checklist rigidly or in isolation to interpret information about a child’s development. It
should be used in conjunction with all developmental information.
Please refer to the “Developmental Milestones and the EYLF and NQS”.
s22(1)(a)(ii) - irrelevant material
Page 13 of 65
s22(1)(a)(ii) - irrelevant material
s22(1)(a)(ii) - irrelevant material
FOI 24/25-1836
s22(1)(a)(ii) - irrelevant material
Developmental Milestones and the EYLF and
External
This information tool can be used in conjunction with other developmental
NQS
information to look for patterns of development and behaviour that may
suggest that a child is or is not developing as expected.
s22(1)(a)(ii) - irrelevant material
Page 17 of 65
FOI 24/25-1836
DOCUMENT 5
Stroke
The content of this document is OFFICIAL
We have received some feedback from external stakeholders in relation to further information
requests being made for people that have recently had a stroke so would like to provide some
practice guidance when it comes to assessing these applications. Please note that the below
information is general information and as usual, each case should be assessed on the
individual information provided:
s22(1)(a)(ii) - irrelevant material
•
In relation to
Section 24(1)(b), we are looking at the permanency of the impairment (in
this case neurological), and not the disability. There are a lot of circumstances where we
receive an application from the treating team advising that the person is still undertaking
rehabilitation, this
does not mean the person automatically doesn’t meet the
permanency criteria. Someone can still be receiving rehabilitation and meet the
permanency criteria, it is important to note that there are no set timeframes we need to
wait before determining that the person has a likely permanent impairment. The aim of
rehabilitation is to improve the
disability that the person is experiencing, however it is
likely that the neurological impairment will be permanent as “a stroke happens when
blood cannot get to your brain, because of a blocked or burst artery. As a result, your
brain cells die due to lack of oxygen and nutrients” (Reference: Stroke Foundation –
What is a Stroke). This therefore meets the NDIAs definition of impairment (outlined in
Our Guidelines- Is your disability caused by an impairment?) as the dead brain cells are
a “loss of, or damage to, a mental function”. Therefore, in line with Sections 5.4 and 5.6
of the NDIS (Becoming a Participant) Rules, we generally could deem a stroke (the
neurological impairment) permanent for one of these reasons:
o
Section 5.4 – The treating team is not recommending any further treatment that
will remedy the neurological impairment (remembering we are looking at the
definition of impairment, not disability)
o
Section 5.6 – Referring to the section in brackets – “the impairment may
continue to be treated and reviewed after permanency has been demonstrated”
– this is applicable when the person is still receiving rehabilitation, however the
treating team expect that they will still live with an impairment post completion
of rehabilitation
s22(1)(a)(ii) - irrelevant material
Page 18 of 65
FOI 24/25-1836
s22(1)(a)(ii) - irrelevant material
Page 19 of 65
s22(1)(a)(ii) - irrelevant material
s22(1)(a)(ii) - irrelevant material
s22(1)(a)(ii) - irrelevant material
s22(1)(a)(ii) - irrelevant material
s22(1)(a)(ii) - irrelevant material
s22(1)(a)(ii) - irrelevant material
s22(1)(a)(ii) - irrelevant material
s22(1)(a)(ii) - irrelevant material
s22(1)(a)(ii) - irrelevant material
s22(1)(a)(ii) - irrelevant material
s22(1)(a)(ii) - irrelevant material
s22(1)(a)(ii) - irrelevant material
s22(1)(a)(ii) - irrelevant material
s22(1)(a)(ii) - irrelevant material


 OFFICIAL
OFFICIAL
FOI
24/25-1836
DOCUMENT 8
Talking Points
The contents of this document are OFFICIAL
Background only – for verbal distribution only. Document strictly not for external distribution.
Update and Reminders Newsletter Edition #20
June 2024
Version control: V1.0 – 18 July 2024
How to use this information
s22(1)(a)(ii) - irrelevant material
Key messages
s22(1)(a)(ii) - irrelevant material
OFFICIAL
Page 51 of 65
FOI 24/25-1836
s22(1)(a)(ii) - irrelevant material
17 July 2024
Page 52 of 65
2
FOI 24/25-1836
s22(1)(a)(ii) - irrelevant material
17 July 2024
Page 53 of 65
3
FOI 24/25-1836
s22(1)(a)(ii) - irrelevant material
17 July 2024
Page 54 of 65
4
FOI 24/25-1836
s22(1)(a)(ii) - irrelevant material
17 July 2024
Page 55 of 65
5
FOI 24/25-1836
s22(1)(a)(ii) - irrelevant material
17 July 2024
Page 56 of 65
6
FOI 24/25-1836
s22(1)(a)(ii) - irrelevant material
Ask Us Anything
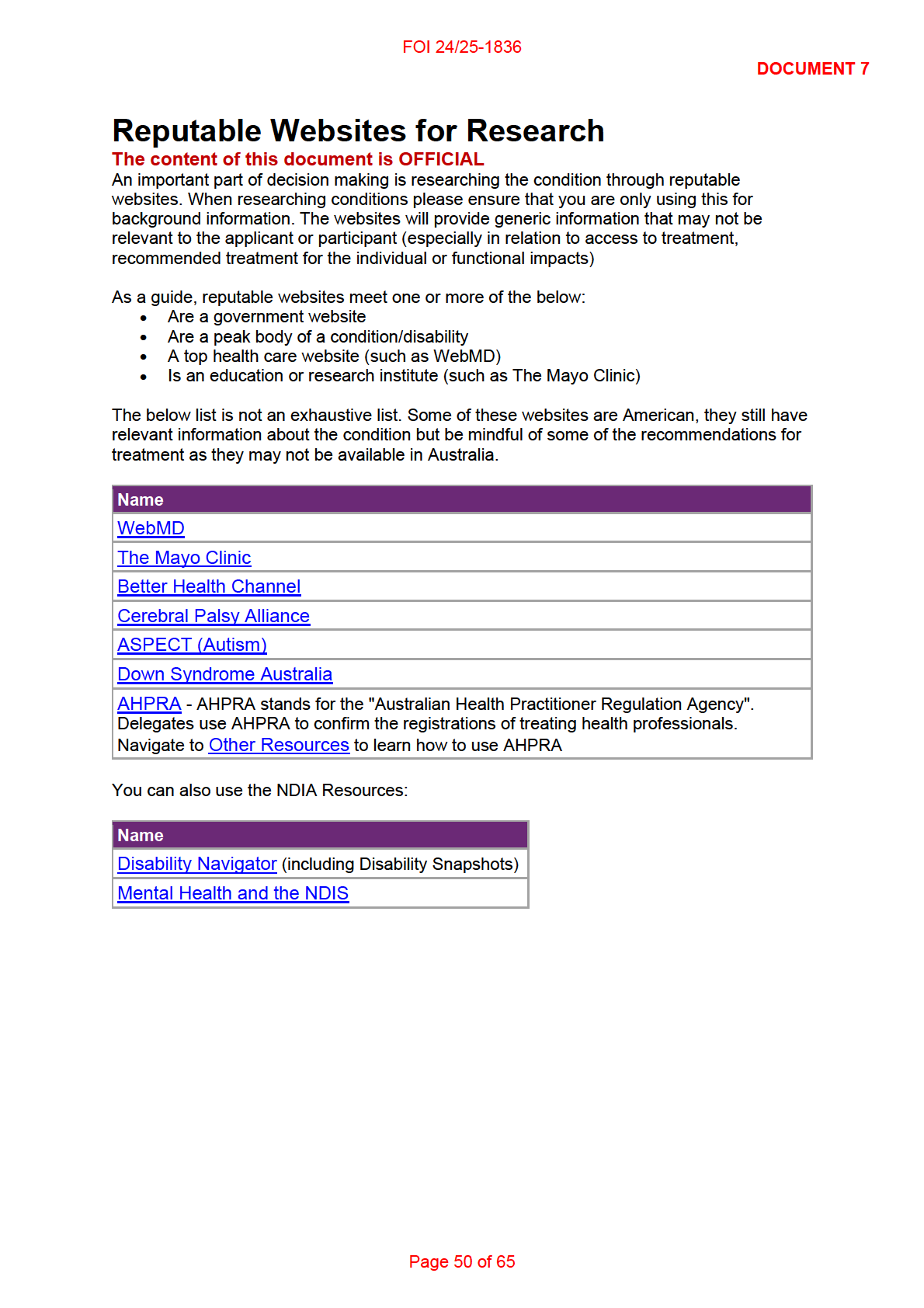
Reliable Sources of Disability Information
• If you’re seeking to broaden your understanding of disabilities, either for personal growth or
your professional role within the Agency, it’s important to refer to reputable websites.
• Reputable websites typically meet one or more of the following criteria:
o They are government websites.
o They are the official sites of peak bodies for a specific condition or disability.
o They are top healthcare websites (such as WebMD).
o They are educational or research institutes (such as The Mayo Clinic).
• One such reputable source in Australia is the peak disability rights and advocacy
organisation, People with Disability Australia (PWDA).
• They provide a range of resources and videos that may be beneficial to staff.
• Staff can also access the NDIA’s Disability Navigator to improve awareness and
understanding of the lived experience of people with disabilities.
• While these resources are excellent for enhancing your understanding, it’s important to
remember that every applicant, participant, and person with a disability is unique.
• Research should serve as a tool to provide you with general information, but it should not
be used to generalise each applicant and their disability.
• Remember, everyone is unique.
What’s your question?
17 July 2024
Page 57 of 65
7
FOI 24/25-1836
s22(1)(a)(ii) - irrelevant material
17 July 2024
Page 58 of 65
8
FOI 24/25-1836
s22(1)(a)(ii) - irrelevant material
17 July 2024
Page 59 of 65
9
FOI 24/25-1836
s22(1)(a)(ii) - irrelevant material
17 July 2024
Page 60 of 65
10
FOI 24/25-1836
s22(1)(a)(ii) - irrelevant material
Page 62 of 65
FOI 24/25-1836
s22(1)(a)(ii) - irrelevant material
Page 63 of 65
FOI 24/25-1836
s22(1)(a)(ii) - irrelevant material
Ask Us Anything
Reliable Sources of Disability Information
If you’re seeking to broaden your understanding of disabilities, either for personal growth or your professional role within the
Agency, it’s important to refer to reputable websites.
Reputable websites typically meet one or more of the following criteria:
They are government websites.
They are the official sites of peak bodies for a specific condition or disability.
They are top healthcare websites (such as WebMD).
They are educational or research institutes (such as The Mayo Clinic).
One such reputable source in Australia is the peak disability rights and advocacy organisation, People with Disability Australia
(PWDA). They provide a range of resources and videos that may be beneficial to staff. These include informative videos on
the Social Model of Disability and a Disability Language Guide. These resources have contributed to the development of the
Australian Government’s Style Manual page on Inclusive Language for People with Disability.
Staff can also access the NDIA’s Disability Navigator to improve awareness and understanding of the lived experience of
people with disabilities.
While these resources are excellent for enhancing your understanding, it’s important to remember that every applicant,
participant, and person with a disability is unique. Everyone’s experience with disability is different. Research should serve as
a tool to provide you with general information, but it should not be used to generalise each applicant and their disability.
Remember, everyone is unique.
What’s Your Question?
If there is anything you would like to know about our branch or agency, you can ask anonymously by completing the Ask Us
Anything Form.
s22(1)(a)(ii) - irrelevant material
Page 64 of 65
FOI 24/25-1836
s22(1)(a)(ii) - irrelevant material
Page 65 of 65