Independent Review of the place of Art
and Music Therapy within Australia’s
National Disability Insurance Scheme
Stephen Duckett AM
April 2025
Issues in this report
Ensuring art and music therapeutic
supports are evidence based
Benefits participants because support
Benefits community because public money
more likely to have an impact
well spent
Make sure everyone who bills as an art or
Need to ensure information about evidence
music therapist is an art or music therapist
is easily accessible
Participants and their advisers
Need to make sure smaller participant
need to know about the evidence
communities are not unfairly excluded
to support participant choices
because of poor evidence base
Need to collect and collate data about
Researchers may not have
outcomes for individual participants to help
developed evidence as it
build the evidence
applies to some communities
Key findings and recommendations
• The key finding of this Review is that the literature provides evidence that art and
music therapy are effective and beneficial to people in some circumstances, for
example where the person has a specific condition and where the therapy is
relevant to their seeking to achieve a specific objective or outcome (paragraph 160).
• Art or music therapy should only be included as a funded therapeutic support in a
participant’s plan if there is generalisable evidence which shows the value of art or
music therapy for similar people with these types of goals and these types of
conditions. It is the responsibility of the National Disability Insurance Agency (NDIA)
to ensure information about the evidence is widely available (paragraph 82).
On evidence
I recommend that the NDIS Evidence Advisory Committee, when established:
• include an assessment of the evidence base for art and music therapy interventions
in specific cohorts in its 2025-26 work plan (paragraph 162).
• considers the concept of a minimal clinically important difference in making its
recommendations (paragraph 142).
• develop explicit processes for making decisions about provision of therapeutic
support in populations where there is a poorly developed evidence base (paragraph
168).
I recommend that the NDIA:
• consider ways in which better information can be provided to participants to assist
them make informed choices about whether particular therapeutic supports could be
a useful, evidence-based addition to their plans (paragraph 104).
• in messaging about evidence, should emphasise the benefits to a cohort of
participants receiving an art or music therapy intervention, distinguishing that from
generic advice about any intervention provided by art or music therapists (paragraph
161).
• strengthen its oversight of plans to ensure that all therapeutic support approved, -
not only in art or music therapy - has a robust evidence base (paragraph 173).
• systematise its collection of data from providers about the effectiveness and
outcomes of therapy interventions for participants, including development of
consistent definitions of interventions aligned to a robust participant outcomes
framework (paragraph 181).
• ensure that data collected by the NDIA is collated and analysed to ensure that the
therapeutic support provided actual y achieves a result for the condition for this
participant with this provider (paragraph 173).
On payments and payment rates
I recommend that the NDIA:
• set rate maxima for art and music therapists on the basis that these are distinct
professions, providing evidence-based therapy, not simply supervising art or music
activities (paragraph 214).
• align the maximum payment limit for art and music therapy with the maximum
payment limit for counsel ors (paragraph 242).
• explore establishing differentials within the allied health professionals’ scales to
recognise different capacity to provide services and/or to recognise levels of skil s
and experience (paragraph 248).
• expand its capacity to monitor market dynamics to assess supply of, and the
demand for, art and music therapy and therapists (paragraph 229).
• In the medium term, set payment limits for art and music therapy that take account
of their labour market monitoring and the need to ensure there is an adequate
supply of art and music therapists to meet the requirement for evidence-based
provision of art and music therapy (paragraph 235).
• consider alternative methods for funding early intervention services which are
consistent with best practice guidelines and any future agreed early childhood
intervention best practice frameworks, which encourage holistic evidence-based and
outcomes-focused provision consistent with the early childhood approach
(paragraph 54).
• consider a different payment and funding approach, particularly for large
organisational providers (paragraph 270).
• specify in its Pricing Arrangements and Price Limits, that art and music therapy
cannot be claimed under ‘other professional’ (paragraph 243).
• ensure that funding for art and music therapy as a Therapeutic Support for self-
managed participants be limited to supports provided by appropriately trained art
and music therapists as defined by NDIA who meet the requirements of NDIS
Quality and Safety Commission registration. In other circumstances, art or music
activities should be classified as Participation in Community, Social and Civic
Activities and funded accordingly (paragraph 251).
• enhance its invoice verification process to ensure that only eligible providers are
reimbursed under the art or music therapy item numbers (paragraph 34).
I recommend that the NDIS Quality and Safeguards Commission
• consider introducing an ongoing mechanism to review the verification requirements
for recognition as an art or music therapist (paragraph 67).
link to page 6 link to page 10 link to page 13 link to page 17 link to page 41 link to page 57
Table of Contents
Introduction ....................................................................................................................... 1
What are art and music therapy? .........................................................................................
5
Early intervention services ..................................................................................................
8
The evidence bases for art and music therapy ....................................................................
12
Pricing and rate setting .....................................................................................................
36
Conclusion ......................................................................................................................
52
link to page 6 link to page 6
Introduction
1. The National Disability Insurance Scheme (NDIS) is one of the most important reforms in
social policy in Australia in recent decades
.1 It was developed so that people with
disabilities are able to participate in Australian society and be provided with the supports
necessary to achieve that.
2. The NDIS was set up to support people with ongoing disabilities (including younger
people who would benefit from early intervention).
3. The NDIS arose because of historic – and, unfortunately, continuing – barriers to
inclusion as noted in a submission to this review:
The NDIS as a support scheme is not needed solely because people have
impairments. It exists equal y as an indictment on the chronic inaccessibility of nearly
all mainstream spaces and services. It costs a lot of money to include Australians
with disability because of serious deficiencies in the skil s, knowledge and flexibility of
our public services, infrastructures and population. You cannot capacity build
disabled individuals out of the barriers they experience when many of those barriers
are the result of environmental conditions, not only individual on
es.2
4. The premise of the NDIS is facilitative, contributing to participants’ achieving their own
goals, with both goals and supports articulated in their individual plans. Plans may also
include goals and supports which are not provided by the NDIS but are the result of
participants’ own choices, and broader community services.
5. The supports which can be funded through the NDIS are specified (‘NDIS Supports’) and
are distinct from ordinary costs of living. Approved NDIS supports include ‘Therapeutic
supports’ defined as
Supports that provide evidence-based therapy to help participants improve or
maintain their functional capacity in areas such as language and communication,
personal care, mobility and movement, interpersonal interactions, functioning
(including psychosocial functioning) and community living.
6. To date art and music therapy have been included as therapeutic supports, but a recent
policy change - since paused – called these services into question, which was in part a
stimulus for this Review.
1 Buckmaster, Luke and Clark, Shannon (2018), 'The National Disability Insurance Scheme: a chronology',
Research Paper (Canberra: Parliament of Australia. Department of Parliamentary Services); Miller, Pavla
and Hayward, David (2016), 'Social policy ‘generosity’ at a time of fiscal austerity: The strange case of
Australia’s National Disability Insurance Scheme',
Critical Social Policy, 37 (1), 128-47.
2 Deafblind Australia Submission to Independent Review of NDIS Art and Music Therapy Supports
1
link to page 7 link to page 7 link to page 7 link to page 7 link to page 7
7. The policy change was made in the context of a ‘rapid revi
ew’3 of the evidence about the
effectiveness of art and music therap
y.4 Rapid reviews are legitimate and a well-
accepted method of research synthesis and have been described as ‘a pragmatic
approach to synthesize evidence in a timely manner.
’5
8. I was asked by the National Disability Insurance Agency (NDIA), which administers the
NDIS, to review two aspects of art and music therapy within the NDIS:
• the NDIA’s ‘review of evidence’, which found that there is limited evidence about
the effectiveness of art and music therapy as evidence-based, therapeutic
supports for most people with disability; and
• the pricing of music and art therapy compared with other allied health therapies.
9. This Report then is about the triad of participants, evidence, and the therapies/therapists,
and how they interact in the interests of the community, especially participants.
10. Australia has a strong history of ensuring that publicly funded services and supports are
evidence-based, starting with the Pharmaceutical Benefits Scheme more than thirty
years ago
,6 and later extending to the Medicare Benefits Schedule. This approach is
being extended to the NDIS and so, in the medium term, identifying whether particular
interventions work for specific cohorts wil be the responsibility of a new Evidence
Advisory Committee in the Department of Social Services, as recommended by the NDIS
Revi
ew.7 The new committee wil draw on evidence about the benefits, quality, safety
and cost-effectiveness of NDIS supports.
11. As part of this review, I invited submissions and received over 600 responses from key
provider associations, Disability Representative and Carer Organisations, individual
participants receiving these services (and their families/carers/advocates), and service
providers.
3 Hamel, Candyce, et al. (2021), 'Defining Rapid Reviews: a systematic scoping review and thematic
analysis of definitions and defining characteristics of rapid reviews',
Journal of Clinical Epidemiology, 129,
74-85.
4 National Disability Insurance Agency. Evidence and Practice Leadership Branch (2024), 'Evidence
Summary: Art and music therapy', (Canberra: NDIA); https://dataresearch.ndis.gov.au/research-and-
evaluation/decision-making-access-and-planning/evidence-summary-art-and-music-
therapy#download-the-evidence-summary
5 Devane, Declan, et al. (2024), 'Key concepts in rapid reviews: an overview',
Journal of Clinical
Epidemiology, 175, 111518.
6 Lopert, Ruth and Viney, Rosalie (2014), 'Revolution then evolution: The advance of health economic
evaluation in Australia',
Zeitschrift für Evidenz, Fortbildung und Qualität im Gesundheitswesen, 108 (7),
360-66.
7 Independent Review into the National Disability Insurance Scheme (2023), 'Final Report: Working
together to deliver the NDIS', (Canberra: The Review).
2
link to page 8
12. Over a fifth of all submissions were from people who identified themselves as
participants or carers. I would like to thank those participants who shared their personal
stories and acknowledge the contributions they are making to improving the NDIS.
13. I also met with the three key associations representing providers of art and music
therapy: the Australian Music Therapy Association, the Australian, New Zealand and
Asian Creative Arts Therapies Association and the College of Creative and Experiential
Therapies of the Psychotherapy and Counsel ing Federation of Australia. I had separate
consultations with NDIS participants.
14. The NDIA provided me with data to help me understand the dimensions of the provision
of art and music therapy and their review of evidence
.8
15. I would like to thank all who made submissions and those who participated in
consultations, and staff at the NDIS who helped me in analysing submissions and
providing data.
Positionality and qualifications
16. My office is on the unceded lands of the Wurundjeri peoples of the Kulin Nation. I
acknowledge my debt to First Nations Australians and pay my respects to Elders past
and present. I acknowledge that First Nations Australians continue to suffer
disadvantage in their access to, and outcomes from, health and disability services. There
is a paucity of evidence about therapeutic supports for First Nations Australians, and I
regret that this review is not able to make targeted evidence-based recommendations
which might improve access or outcomes for First Nations Australians.
17. I am a white male and no one in my immediate family participates in the NDIS. I have
attempted to address my positionality by reading carefully all the submissions to this
review and listening to the experiences of people with disability as presented to the
review.
18. I bring to this Independent Review internationally recognised expertise in pricing of public
services, particularly health care, a deep understanding of the way governments and
public services operate, a history of management and policy achievements, and a
lifelong commitment to equity, efficiency, and quality of service provision.
8 National Disability Insurance Agency. Evidence and Practice Leadership Branch (2024), 'Evidence
Summary: Art and music therapy', (Canberra: NDIA).
3
link to page 9 link to page 9
19. My prior experience with disability services and the NDIS has been partly through
employment and board roles. In the Victorian Department of Health and Community
Services in the early 1990s I had line responsibility for two rural regions at different times
and so had responsibility for all Departmental services in the regions, including disability
services. As Secretary of the Commonwealth Department of Human Services and
Health, also in the 1990s, I had responsibility for aspects of disability services. I am also
a former board member of the Brotherhood of St Laurence, which provided local area
coordination and early intervention advice under contract to the NDIA. When I was Dean
of Health Sciences at La Trobe University, the Faculty included education for art therapy.
20. I have maintained a general interest in aspects of disability policy and services and have
co-authored a number of publications on aspects of measurement relating to disability
and therapy supports
.9 I also included a review of disability services in my book on the
Australian health care system
.10
9 Dyson, M., Allen, F.C.L., and Duckett, S.J. (2000), 'Profiling childhood disability: The reliability of the
educational needs questionnaire',
Evaluation and Program Planning, 23 (2), 177-85; Dyson, M., Duckett,
S.J., and Allen, F.C.L. (2000), 'A therapy-relevant casemix classification system for school age children
with disabilities',
Archives of Physical Medicine and Rehabilitation, 81 (May), 634-43; Morris, M., et al.
(2005), 'Reliability of the Australian Therapy Outcome Measures for quantifying disability and health',
International Journal of Therapy & Rehabilitation, 12 (8), 340-46; Perry, Angela, et al. (2004), 'Therapy
outcome measures for allied health practitioners in Australia: the AusTOMs',
International Journal of
Quality in Health Care, 16 (4), 285-91; Unsworth, Carolyn A., et al. (2004), 'Validity of the AusTOM scales:
A comparison of the AusTOMs and EuroQol-5D',
Health and Quality of Life Outcomes, 2 (64), 1-12.
10 Duckett, Stephen (2022),
The Australian Health Care System (6th ed.) (Melbourne: Oxford University
Press).
4
link to page 10 link to page 10
What are art and music therapy?
21. Art and music therapy are increasingly recognised as important potential contributors to
improving the life situation for people across a broad range of condition
s.11
22. The Australian, New Zealand and Asian Creative Arts Therapies Association
(ANZACATA) describes art therapy as the use of ‘art, media and the creative process
(drawing, writing, sculpting, drama, clay, sand, dance and movement) to facilitate the
exploration of feelings, improve self-awareness and reduce anxiety for clients.’
23. Art therapists are not registered as part of Australia’s national system of registering
health professionals. However, to provide therapeutic supports funded by the NDIS an
art therapist must, among other things, be a ‘professional member’ of ANZACATA.
24. Professional members of ANZACATA are required to have a master’s degree in art
therapy approved by ANZACATA.
25. The Australian Music Therapy Association (AMTA) defines music therapy as ‘the
intentional and therapeutic use of music by registered music therapists (RMTs) to
support people to improve their health, functioning and wel being’. Aalbers et al.
identified two types of music therapy: ‘active (where people sing or play music) and
receptive (where people listen to music)
’.12
26. Music therapists are also not registered as part of Australia’s national system of
registering health professionals, but AMTA is a member of the National Al iance of Self-
Regulating Health Professions.
27. To be a registered music therapist endorsed by AMTA, a person must complete a
master’s degree course approved by AMTA. To provide therapeutic supports funded by
the NDIS a music therapist must, among other things, be a ‘registered music therapist’
with AMTA.
11 World Health Organization. Regional Office for, Europe (2023), 'WHO expert meeting on prevention and
control of noncommunicable diseases: learning from the arts. Opera House Budapest, Hungary, 15–16
December 2022: meeting report', (Copenhagen: WHO Regional Office for Europe).
12 Aalbers, Sonja, et al. (2017), 'Music therapy for depression',
Cochrane Database of Systematic Reviews, 11, CD004517. Davies and Clift make the same distinction about types of arts engagement: Davies,
Christina R. and Clift, Stephen (2022), 'Arts and Health Glossary - A Summary of Definitions for Use in
Research, Policy and Practice',
Frontiers in Psychology, 13 (949685), 1-6.
5
link to page 11 link to page 11
28. A consequence of neither art nor music therapy being nationally registered professions is
that there is no protection of those titles, so anybody can call themselves an ‘art
therapist’ or a ‘music therapist’. However, as indicated above, the NDIS rules prescribe
who ought to be able to claim the relevant item numbers.
29. In 2023-24 about 13,400 people were supported by the NDIS for one of these services,
and 600 who received both.
Table 1: Number of art and music therapy participants and providers, 2023-24
Art therapy
Music therapy
Number of participants
6,788
7,217
Number of providers
1,672
1,405
Total payments
$ 13.4m
$ 16.3m
Source: NDIA administrative data provided to this review; Note: Data in this table (and in
subsequent tables and figures) may not include full information about supports provided to
self-managed participants.
30. There is some evidence that people receiving music therapy tend to be younger than
those receiving art therapy. About one in five people receiving music therapy are under
9, compared to one in seven receiving art therapy (21% v 14%). Conversely, about 37%
of those receiving art therapy are 35 or over compared to 30% of those receiving music
therapy. However, the NDIS data does not allow for the identification of usage of art and
music therapy for under 7s as those services are claimed under a general therapy code.
31. Again, subject to the issue about under 7s above, about two thirds of people who receive
art therapy are women or girls. The gender balance is reversed for music therapy: 40%
of people who receive music therapy are women or girls
.13
32. The number of separate art or music therapy providers paid under the NDIS appears to
be larger than the membership base of the relevant associatio
ns.14
33. Art or music
therapy are not the same as art or music
activities:
•
Art or music therapy: Supports that formally implement elements of art or music
as therapeutic techniques alongside or instead of psychotherapy, physiotherapy,
speech therapy and rehabilitation. To be considered art or music therapy, a
service must meet all the following criteria: Art or music therapy is delivered by a
13 I was not provided with data on the number of non-binary participants.
14 The data on number of providers is based on number of unique ABN codes. It is possible that a therapist
may bill using two or more ABNs, for example, to distinguish sites of care.
6
qualified art or music therapist (typically prepared at master’s level); implements
a clearly defined and scientifically valid mechanism of action; and aims at an
identified and measurable outcome beyond leisure, such as psychosocial
functioning, physical capacity or communication.
•
Art or music activities: Services that involve art or music but do not meet al of the
criteria of art or music therapy, even if delivered by a qualified art or music
therapist or involve therapeutic techniques. These are mainly aimed at leisure or
use art or music to facilitate other benefits such as social interactions or
movement.
34.
I recommend that the NDIA enhance its invoice verification process to ensure that
only eligible providers are reimbursed under the art or music therapy item
numbers.
7
link to page 13 link to page 13
Early intervention services
35. There are two pathways into the NDIS – early intervention for younger people and the
general permanent disability stream. Most of what I have to say in this report relates to
the larger element of the NDIS, permanent disability and supports for this group of
participants.
36. The purpose of early intervention is to mitigate the impact of a person's impairment upon
their long-term functional capacity by providing support at the earliest possible stage.
Early intervention support is also intended to benefit a person by reducing their future
need for supports and by strengthening the sustainability of their informal supports, e.g.
building the capacity of their carer(s)
.15
37. A draft National Best Practice Framework for the provision of early childhood
intervention, drawing on an extensive literature review and a review of best practice, is
currently being developed
.16 A major theme of the best practice framework for early
intervention is the importance of being child-and family-centred and outcomes-focused.
38. The draft Framework applies across all areas of early childhood intervention and so is
not NDIS-specific. If the Framework is seen as relevant and useful by stakeholders,
there would be merit in its being used to shape NDIS provision.
39. Best practice early childhood intervention identifies the desired outcomes and then the
most effective interventions consistent with the principles that underpin the framework.
The key questions are: What are the likely gains in function and meaningful participation
in everyday settings of childhood? Are the gains greater than alternative interventions or
are the gains sufficiently effective in combination with other interventions so as to be
attractive? If the therapy is used but does not lead to improved functioning and
meaningful participation in the child, it should not continue to be used.
40. In terms of my commission, to examine the evidence base for art and music therapy, the
review of best practice points to how art and music therapy ought to be provided as part
of early childhood intervention services, namely in the context of implementation of this
(draft) evidence-based National Best Practice Framework.
15 Imms, Christine, et al. (2024), 'Review of best practice in early childhood intervention: Desktop review
full report.' (Melbourne: The University of Melbourne).
16 The Framework is being developed by a broad group including a number of stakeholders. It was
commissioned by the Department of Social Services. The University of Melbourne (2025), 'Review of best
practice in early childhood intervention: Draft Practice Framework v2.0', (Melbourne: The University of
Melbourne).
8
link to page 14 link to page 14 link to page 14 link to page 14
41. However, there are elements of the overall funding design of the NDIS which may
militate against the implementation of the themes of the (draft) National Best Practice
Framework.
42. The current funding arrangements for provision of paediatric speech and language were
reported in a recent study as not consistent with the evidence, although the relevant
papers did not explore the nature of the inconsistency, nor point to specific directions for
reform
.17
43. A small qualitative study conducted in the early stages of the implementation of the
NDIS, identified several themes about its then negative impact on early childhood
intervention services. It identified that sometimes the parents felt disempowered
compared to previous systems and emphasised the importance of good information for
families
.18 It also concluded that the NDIS funding arrangements – essential y fee-for-
service – may have inhibited good service provision.
44. Use of a ‘key worker’ to coordinate services may address some of the problems
identified with early childhood intervention service
s,19 however, involvement of a key
worker is not universal.
45. This Review cannot address all of the issues involved in the development of early
childhood intervention policy. However, my observation is that the atomised approach,
based on separate funding for separate therapeutic supports is not conducive to
encourage the policy directions set out in the draft National Best Practice Framework,
and hence does not facilitate evidence-based provision in this context.
46. In the health sector there is increasing recognition of the importance of multidisciplinary
teams in the provision of health care, especially for older people. The same is true for
early intervention for all people with disability. In the health sector, the response is to
recognise the limitations of fee-for-service payments and to encourage holistic payments
which encourage continuity of care and the right mix of services being provided to the
person in need
.20
17 Nickless, Tristan, et al. (2023), 'Public purse, private service: The perceptions of public funding models
of Australian independent speech-language pathologists',
International Journal of Speech-Language
Pathology, 25 (3), 462-78; Nickless, Tristan, et al. (2024), 'Aligned or misaligned: Are public funding
models for speech-language pathology reflecting recommended evidence? An exploratory survey of
Australian speech-language pathologists',
Health Policy OPEN, 6, 100117.
18 Gavidia-Payne, Susana (2020), 'Implementation of Australia's National Disability Insurance Scheme:
Experiences of Families of Young Children with Disabilities',
Infants & Young Children, 33 (3), 184-94.
19 Young, Dana, et al. (2021), 'Understanding key worker experiences at an Australian Early Childhood
Intervention Service',
Health & Social Care in the Community, 29 (6), e269-e78.
20 Strengthening Medicare Taskforce (2023), 'Report', (Canberra: Department of Health and Aged Care).
9
link to page 15 link to page 15
47. The same principles might apply for early intervention services. Here one might see
payment for a multidisciplinary team, with the expectation that the multidisciplinary team
provides holistic support to achieve agreed outcomes for a specified number of people in
the early intervention stream for a defined time. e.g., a year. People should have the right
to change providers to ensure appropriate accountability and responsiveness with a
specified notice period.
48. Such a holistic approach might be more difficult to organise in rural and remote Australia,
where the numbers involved are small, but it might be possible to link up with local
community services who are able to provide support, especially with remote guidance to
those teams provided virtual y. This was recommended by the NDIS Review
.21
49. Provision of early childhood intervention services in this model might also be through a
procurement approach, where potential providers respond to an open invitation to
participate based on their capabilities and ability to provide services consistent with the
National Best Practice Framework when finalised and as updated from time to time.
50. It is important to note that the draft National Best Practice Framework is just that, a draft.
It has not yet been adopted as policy and may not be. But if it is adopted, then it is
important that funding and policy aspirations are aligned, lest the Framework simply be
another statement of unimplemented aspirations.
51. Funding of multi-disciplinary teams is not simple valorising use of a ‘multi-disciplinary
team’ item. It is about facilitating a service which involves true teamwork, on an ongoing
basis, in the interest of the participant, with appropriate accountabilities
.22
52. What I am pointing to here is not a return to block funding, which was associated with a
lack of accountability to clients, but rather that existing fee-for-service funding
arrangements do not serve participants well and may stymie implementation of a new
National Best Practice Framework if adopted.
53. In this model, perhaps termed ‘team funding’, participants would be empowered by being
able to move between teams/providers if their needs were not being met. Under this
arrangement the NDIA would augment its existing oversight by monitoring participant
reported experience measures, and tracking outcomes.
54.
I recommend that the NDIA consider alternative methods for funding early
intervention services which are consistent with best practice guidelines and any
21 Independent Review into the National Disability Insurance Scheme (2023), 'Final Report: Working
together to deliver the NDIS', (Canberra: The Review).
22 Katzenbach, Jon R and Smith, Douglas K (2005), 'The discipline of teams',
Harvard business review, 83
(7/8), 162-71.
10
link to page 16
future agreed early childhood intervention best practice frameworks, which
encourage holistic evidence-based and outcomes-focused provision consistent
with the early childhood approach. In the interim, the NDIA should continue to fund
early childhood intervention supports in a flexible budget which promotes a best practice
approach consistent with best practice guidelines in early childhood intervention
.
55. As part of foundational supports, states might give consideration to professional
development for teachers and early childhood educators to work with music and art
therapists to build their capability and confidence in provision of programs which draw on
art or music therapy evidence
.23
56. Unless otherwise specified, the remainder of this report does not consider the evidence
base for, or pricing of, early intervention services for children or other groups.
23 Ng, Siu-Ping, et al. (2024), 'Impact of online professional development on Hong Kong kindergarten
teachers' confidence: An experimental study',
Australian Journal of Music Education, 56 (2), 52-64.
11
The evidence bases for art and music therapy
57. A number of stakeholders, including the three main provider associations provided
comprehensive submissions highlighting the evidence base for art or music therapy. As
discussed below, I received more than 150 submissions from participants and/or carers,
many of them recounting their personal experience of the benefits of art or music
therapy. Some of these also pointed to relevant literature for me to consider.
AMTA submission
58. AMTA provided a comprehensive submission (including appendices directing me to
relevant studies). AMTA identified from the literature a number of areas where music
therapy might be of benefit:
•
Functioning (including psychosocial functioning): Here AMTA concluded that ‘A
range of music therapy methods, techniques and interventions are examined in
the research literature, including therapeutic singing and instrument play,
rhythmic cueing, music assisted storytelling, dyadic improvisations, receptive
methods, therapeutic song writing and composition, music and movement, and
musical play. Research evidence shows a range of outcomes relevant to this
domain across various focus areas that relate to functioning, including global
cognition, attention, memory, recal , auditory discrimination, music engagement,
depression, anxiety, mood, and apathy’;
•
Language and communication: AMTA noted that ‘Music therapy evidence
demonstrates improvements in a range of functional language and
communication domains. Improvements for people who wil be able to develop or
recover language are obviously more amenable to quantitative measurement.
This is seen by significant improvements in people with aphasia after music
therapy as demonstrated through meta-analysis;
•
Interpersonal Interactions: AMTA identified that in this field ‘participants with
primary impairments of either neurological or psychosocial types are the most
common (18 and 16 citations respectively), and research with children and
adolescents is prominent (32 citations). There are 19 systematic reviews or meta-
analyses that are relevant to this area; and
•
Mobility and movement: The AMTA summary showed ‘A total of 26 citations
exploring the role of music therapy in improving movement and mobility functional
capacity have been selected for this summary. These studies explore music
therapy movement interventions for people experiencing impairments in the
NDIA-related domains of neurological functioning (18 citations), physical
functioning (5 citations) and cognitive functioning (3 citations)’.
59. AMTA also noted that music therapy can offer benefits relating to
community living but
the evidence base overlaps other areas.
12
link to page 18 link to page 18 link to page 18
60. The AMTA analysis is structured according to functional domains. Within each of these
functional domains, systematic reviews look at specific conditions such as aphasia
.24 The
critical issue for establishing an evidence based is therefore the interaction of the
condition and the functional domain.
ANZACATA submission
61. Although grouped together in this Review, art and music therapy have both similarities
and differences. The definition of music therapy cited above highlights the use of music
as an intervention. In contrast, the definition of art therapy highlights arts as a medium
which allows the intervention which is the exploration of feelings.
62. The ANZACATA submission therefore drew my attention to the evidence base for the
psychological literature as published by the Australian Psychological Society
,25 with the
assumption being that art therapists use the relevant range of psychological
interventions.
63. ANZACATA also provided a survey of the literature relating to art therapy specificall
y.26
64. Again, both the general and specific literature is structured according to the evidence for
specific conditions, with literature for one functional domain – cognition – identified in the
art therapy specific literature review.
PACFA CCET submission
65. The Col ege of Creative and Experiential Therapists of the Psychotherapy and
Counsel ing Federation of Australia (PACFA CCET) also made a submission. The
evidence table of their submission covered much the same ground as AMTA’s and
ANZACATA’s.
66. PACFA CCET also argued that accreditation through their processes should be
recognised under the NDIS arrangements.
67.
I recommend that the NDIS Quality and Safeguards Commission consider
introducing an ongoing mechanism to review the verification requirements for
recognition as an art or music therapist.
24 Liu, Qingqing, et al. (2022), 'The effect of music therapy on language recovery in patients with aphasia
after stroke: a systematic review and meta-analysis',
Neurological Sciences, 43 (2), 863-72.
25 Australian Psychological Society (2024), 'Evidence-based psychological interventions in the treatment
of mental disorders: A literature review', (Melbourne: APS).
26 Gray, Deanne (2022), 'The Proven Efficacy of Creative Arts Therapies: What the Literature Tells Us',
(North Brighton: ANZACATA).
13
link to page 19 link to page 19
Disability Representative and Carer Organisations
68. Several Disability Representative and Carer Organisations made helpful submissions to
this review and also provided evidence of the benefit of art or music therapy for
participants with specific condition
s.27
Towards a learning organisation
69. The NDIA should strive to be a learning organisation. This is not just jargon but is a
guiding principle that strives to both improve care provided and contribute to the body of
evidence on which care is based. A learning organisation is ‘an organization skil ed at
creating, acquiring, and transferring knowledge, and at modifying its behaviour to reflect
new knowledge and insights’
.28
70. The world around us is changing and new knowledge is being created all the time. It is
critical that NDIS participants benefit from that new knowledge as quickly as possible,
whether it is knowledge about new interventions which have been shown to make a
difference and so need to become available to all participants, or knowledge about old
practices which have been shown not to make a difference and need to be discarded as
giving false hope and costing money.
71. The NDIA should become more adept at gathering data – including data on the
experience of NDIS participants – and using data to inform the plan development and
approval process. It should be at the forefront of synthesising evidence to inform its
decisions and is a theme of this review.
27 e.g., Dementia Australia Independent Review of NDIS art and music therapy supports: A Dementia
Australia Submission
28 Garvin, David A (1993), 'Building a Learning Organization',
Harvard Business Review, 71 (4), 78-91.
14
link to page 20 link to page 20
What is evidence?
72. Section 3.2 of the
National Disability Insurance Scheme (Supports for Participants) Rules
2013 states that
In deciding whether the support wil be, or is likely to be, effective and beneficial for a
participant, having regard to current good practice, the CEO (of the NDIA) is to
consider the available evidence of the effectiveness of the support for others in like
circumstances. That evidence may include:
• published and refereed literature and any consensus of expert opinion;
• the lived experience of the participant or their carers; or
• anything the Agency has learnt through delivery of the NDIS.
73. Further, published NDIS guidance, states that
Therapeutic supports under the NDIS are limited to ‘supports that provide
evidence-
based therapy’ (emphasis added).
74. The NDIS Quality and Safeguards Commission has produced an ‘Evidence Informed
Practice Guide’ which portrays evidence informed practice as being shaped by the rights
and perspectives of the person with disabilities; best research and evaluation evidence;
clinical and provider expertise; and information from the implementing or practice
context
.29
75. Schalock defined evidence-based practices as ‘practices for which there is a
demonstrated relation between specific practices and measured outcomes
.’30 I wil return
to the meaning of ‘demonstrated relation’ later.
76. What is critical is how do the different types of knowledge and evidence interact? It is
appropriate to use different types of evidence at different stages of a participant’s plan
development and implementation journey, making the way the NDIS Guidance and the
Schalock definition are phrased somewhat problematic.
77. Firstly, what is regarded as ‘evidence’ needs to be considered from the perspective of
both the system and the individual.
78. In my view, to meet the evidence criterion in the NDIS definition there should be rigorous
studies which show that for this type of client, the support (art or music therapy) achieves
a measurable result. As art and music therapy in Australia is influenced by developments
29 NDIS Quality and Safeguards Commission (2023), 'Evidence-Informed Practice Guide', (Penrith, NSW:
The Commission).
30 Schalock, Robert L., et al. (2017), 'Evidence and Evidence-Based Practices: Are We There Yet?',
Intellectual and Developmental Disabilities, 55 (2), 112-19. page 115
15
link to page 21 link to page 21
internationally in these professions, the evidence synthesis of the effectiveness of these
therapies should draw on international replicable evidence.
79. For an individual participant, this approach to the use of evidence is prospective, that is,
as a participant's plan is being developed, there is research evidence available which
shows that art or music therapy has the potential to benefit this individual. This then can
inform the plan for the participant.
80. What is important here is that the evidence being considered is reproducibl
e,31 both in
the sense that another study looking at the same issue wil most likely come to the same
conclusion, but also that given this study, we can presume that this NDIS participant wil
likely benefit from this intervention
.32
81. That is, synthesis of the research evidence wil enable the Department of Social Services
and the NDIA, on the advice of the new NDIS Evidence Advisory Committee, to form a
view about the effectiveness of that intervention for that participant cohort group with
similar goals. There wil always be a judgement here, as the population in research
studies may never mirror exactly the NDIS participant population, but what is critical is
that participants know what is likely to work for them, based on the best available
evidence, and so how their packages should be used. Similarly, sustainability of the
NDIS means that it is important that the NDIA knows what is likely to have a beneficial
effect for participants.
82. Specifically, subject to the caveats discussed later,
art or music therapy should only
be included as a funded therapeutic support in a participant’s plan if there is
generalisable evidence which shows the value of art or music therapy for similar
people with these types of goals and these types of conditions. It is the
responsibility of the NDIA to ensure information about the evidence is widely
available, an issue to which I wil return.
83.
In addition, therapists should monitor a person’s progress in response to the therapy
provided to ensure that,
in this instance, a measurable and meaningful result is being
achieved. That is, if the therapist’s proposed treatment plan is implemented, the literature
wil show (prospectively) that art or music therapy may benefit this individual because of
the experience of providing these supports in the past to others in a similar situation.
What we now need to know retrospectively is whether the support works as provided by
31 Foley, Thomas and Horwitz, Leora I. (2025) Learning Health Systems [online text], Cambridge University
Press, page 6
32 Relatively new UK guidance is useful here: Skivington, Kathryn, et al. (2021), 'A new framework for
developing and evaluating complex interventions: update of Medical Research Council guidance',
BMJ, 374, n2061.
16
link to page 22 link to page 22 link to page 22 link to page 22
this therapist to
this person in
this context. ‘Result’ here would be outcomes as
contemplated in an individual’s goals and would be different from the person’s previous
situation and trajectory.
84. This type of evidence is retrospective. That is, only after a participant has received
therapeutic supports is it possible to measure the impact of those supports.
85. Although there are common measures of outcomes of provision of therapeutic support,
both covering multiple therapi
es33 and discipline specific, each clinician has autonomy in
determining which measures to use, and how often.
86. Overtime there should be more systematisation of how information on a participant’s
progress and outcomes are collected, collated, and analysed. This wil help build an
evidence base where none exists today and is a key component of building a learning
organisatio
n.34 I wil return to this issue of reporting later.
87. Other types of evidence, such as professional judgement, might also be considered but
that itself must be evidence based, supported by the literature. Again, the clinician or
technical advisor has autonomy to determine what they might recommend as the best art
or music therapy intervention for this person at this time. The clinician or technical
advisor here would draw on their own professional experience and knowledge of the
evidence and their understanding of the participant’s situation and goals.
88. During this review, I received many personal testimonies from people with disabilities,
their carers, or advocates, which attest to the benefit to those individuals of art or music
therapy
.35 Similarly, I received many submissions from therapists who recounted
appropriately anonymised stories about the benefits of the therapy they provided. I also
saw several anonymised professional reports produced by art or music therapists
documenting the progress made while individual participants were receiving these
therapies. Stakeholders also provided me with vignettes showing the benefits of the art
or music therapeutic supports provided to individual participants. There are also
published papers describing case studies of the outcomes of art and music therapy
.36
89. One cannot but be moved by these stories.
33 Perry, Angela, et al. (2004), 'Therapy outcome measures for allied health practitioners in Australia: the
AusTOMs',
International Journal of Quality in Health Care, 16 (4), 285-91.
34 Foley, Thomas and Horwitz, Leora I. (2025)
Learning Health Systems [online text], Cambridge University
Press.
35 I also heard stories where music therapy was not useful, indeed said to be detrimental.
36 Thompson, Grace A. and McFerran, Katrina Skewes (2015), 'Music therapy with young people who have
profound intellectual and developmental disability: Four case studies exploring communication and
engagement within musical interactions',
Journal of Intellectual & Developmental Disability, 40 (1), 1-11.
17
link to page 23 link to page 23 link to page 23 link to page 23
90. I heard firsthand of the difference art or music therapy can make in those individual
circumstances, not only to the person with disabilities but also to those around them.
Unfortunately, support for people with disabilities is stil quite gendered in Australia: in
2022 6.1 per cent of women were primary carers, compared to 3 per cent of men
,37 so
there is a gender equity issue at play here too.
91. The personal statements in submissions and in the consultations address the second
limb of my proposed approach to ‘evidence-based’.
92. That we see change in participants associated with provision of therapeutic supports is
real y no surprise. There is now a substantial – and growi
ng38 - literature, including
systematic reviews, and in the case of music therapy, summaries of
,39 and systematic
reviews of, systematic review
s,40 which outline the benefit of art or music therapy in
specific circumstances, or for people with specific conditions.
93. Although the individual stories shared with me show that there was generally a benefit to
those individuals, they don’t show
in a systematic way whether an alternative support (or
alternative supports) might have provided the same benefit, or whether a different
approach to art or music therapy (e.g. facilitating the carer) might have achieved the
same (or lesser or greater) benefit. Of course, there were some stories which described
how all these other therapies had been tried but no progress was being made until art or
therapy was provided. But it is hard to put these together in a systematic pattern to make
an evaluative assessment.
94. These stories, of prior failure and subsequent progress, raise the question of why art or
music therapy was not provided earlier? If there is evidence that art or music therapy is
beneficial, why was it not part of the original package right from the start?
95. This may not be an issue unique to art or music therapy. But the therapeutic supports
considered in this review are provided by professions which are relatively small
compared to other allied health disciplines, and so the local area coordinator or other
places where participants may gather information, may not be aware of whether these
37 Australian Bureau of Statistics (2024),
Disability, Ageing and Carers, Australia: Summary of Findings
(Canberra: ABS). The data are for people supporting both older people and younger people with
disabilities.
38 Rodriguez Novo, Natalia, et al. (2021), 'Trends in Research on Art Therapy Indexed in the Web of
Science: A Bibliometric Analysis',
Frontiers in Psychology, 12 (752026), 1-10.
39 Kamioka, Hiroharu, et al. (2014), 'Effectiveness of music therapy: a summary of systematic reviews
based on randomized controlled trials of music interventions',
Patient Preference and Adherence, 8 (null),
727-54.
40 Wu, Jiaming, Zhang, Qing, and Wu, Aihong (2024), 'Functioning, health and developmental benefits of
music interventions for children and adolescents with intellectual and developmental disabilities: a
systematic review of systematic reviews',
Chinese Journal of Rehabilitation Theory and Practice, 543-53.
18
link to page 24 link to page 24 link to page 24 link to page 24 link to page 24
therapeutic supports might make a difference in these cases, or even of the existence of
these therapeutic supports at all.
96. The essence of the NDIS is that participants should have choice and control over what
mix of supports wil best help them achieve their goals, so goal setting is fundamental.
But so too is identifying what therapeutic support wil help in achieving those goals, and
good information about what is likely to be effective is necessary for this purpose.
97. A defining characteristic of a market – where they exist – is that consumers in that
market have enough information to choose among the products on offer. Imbalance in
the knowledge of consumers vis-à-vis providers, is referred to as ‘information asymmetry’
and leads to market failure
.41
98. Information asymmetry is not the only reason for market failure, for example, in parts of
Australia there may not be an adequate supply of professionals and other staff to meet
needs, a situation sometimes described as ‘thin markets’
.42
99. Al this points to the need for active ‘market stewardship’ rather than simple market
regulation
,43 or hoping that markets wil work their magic without any superintendence.
There is thus an important role of ‘market stewards’
,44 such as the NDIA and the NDIS
Commission, including in ensuring there is adequate information to participants to make
informed choices
.45
100. There is known to be a long gap – measured in years but estimates and methods for
estimating the length of the gap vary – between new knowledge about treatments in
41 Giza, Wojciech (2024), 'Asymmetric information as a market failure in retrospect
The Elgar Companion to Information Economics', in Daphne R. Włodarczy Raban, Julia (ed.),
The Elgar
Companion to Information Economics (Cheltenham, UK: Edward Elgar Publishing), 106-17.
42 Reeders, Daniel, et al. (2019), 'Market Capacity Framework: An approach for identifying thin markets in
the NDIS', (Sydney: Centre for Social Impact:).
43 Carey, Gemma, et al. (2018), 'The Vexed Question of Market Stewardship in the Public Sector:
Examining Equity and the Social Contract through the Australian National Disability Insurance Scheme',
Social Policy & Administration, 52 (1), 387-407.
44 Independent Review into the National Disability Insurance Scheme (2023), 'Final Report: Working
together to deliver the NDIS', (Canberra: The Review).
45 In the longer term, market regulation in the NDIS needs to reconcile the individualistic/personalism
view of participants in a market and the contemporary public policy concept of co-design and co-
creation, see, for example, Ongaro, Edoardo, Rubalcaba, Luis, and Solano, Ernesto (2025 (in press)), 'The
ideational bases of public value co-creation and the philosophy of personalism: Why a relational
conception of person matters for solving public problems',
Public Policy and Administration, 0 (0),
09520767251318127.
19
link to page 25 link to page 25 link to page 25 link to page 25 link to page 25 link to page 25
health care and implementation in practi
ce.46 Inclusion of research syntheses in
published guidelines helps but is not a panacea
.47
101. There also appears to be a research-practice gap in disability
.48 An essential step in
addressing the gap is that the new Evidence Advisory Committee, as part of its
determination of the evidence and formulating its recommendations, develop a ‘plain
language’ synthesis/summary of its conclusion
s.49
102. However, mere publication of the evidence of what works, even in a plain language
version, wil not be enough to ensure that participants know when to include art or music
therapy in their plans, and art or music therapists know what the latest available
evidence-based interventions are.
103. Again, it is in the best interests of participants and the sustainability of the NDIS, to
ensure good advice is available to help participants, their carers, and their advocates
make informed decisions about what is likely to make a difference. Evidence updates
might also be provided to therapists.
104.
I recommend that the NDIA consider ways in which better information can be
provided to participants to assist them make informed choices about whether
particular therapeutic supports could be a useful, evidence-based addition to their
plans.
105. Ideally, information would be made available in a tailored way, specifying in plain
language that for this type of domain and for a person with this condition, whether there
is evidence that art or music therapy can help achieve their goals
.50
106. In a quite different context
,51 the University of York has a good website which
provides information about potential outcomes of some types of surgery, taking into
46 Evensen, Ann E., et al. (2010), 'Trends in publications regarding evidence-practice gaps: A literature
review',
Implementation Science, 5 (11), 1-5.; Hanney, Stephen R., et al. (2015), 'How long does
biomedical research take? Studying the time taken between biomedical and health research and its
translation into products, policy, and practice',
Health Research Policy and Systems, 13 (1), 1-18.
47 Freitas de Mel o, Nicole, et al. (2024), 'Models and frameworks for assessing the implementation of
clinical practice guidelines: a systematic review',
Implementation Science, 19 (59), 1-15.
48 Dew, Angela and Boydell, Katherine M. (2017), 'Knowledge translation: bridging the disability research-
to-practice gap',
Research and Practice in Intellectual and Developmental Disabilities, 4 (2), 142-57.
49 I use ‘plain language’ throughout this Report rather than ‘plain English’ to recognise the need for
materials in languages other than English.
50 Perhaps a matrix format could be used, but this might be challenging to develop in a plain language
format.
51 The point of this paragraph is to draw attention to a user-friendly way of presenting data to facilitate an
informed choice. Unlike the example used, which is about acute care, participants in the disability stream
have permanent disabilities. That is not to say, of course, that outcome measures are not relevant.
20
link to page 26 link to page 26
account the characteristics of the individual
.52 The data behind the pictorial display used
is drawn from before and after Patient Reported Outcome Measures completed by
patients who have had that type of surgery. I am not aware of anything similar to this to
help people develop their plans under the NDIS. If it were, participants could have advice
specific to their situation to answer the critical question: If art or music therapy (or any
other therapy for that matter) were added to my plan, what might I expect? This type of
analysis could also be developed using data both from the literature and analysis of
individual participant reports submitted to the NDIA, potential y following revision to
standard templates for therapists’ reports on participant progress
.53
107. The second problematic element of the phrasing of ‘evidence based’ is that one
might infer that art or music therapy is provided out of an overall therapeutic context of
the participant.
108. The point of art and music therapy is to contribute to achieving the functional
outcomes and goals established by and for the individual receiving those services. They
should not be conceived of as part of a smorgasbord approach to achieving goals (one
of those, and one of those), but rather as an integrated, holistic approach.
109. The emphasis of the NDIS is, and should be, that supports in combination are to
achieve the individual’s goals. Art or music therapy may, subject to the evidence, be
appropriate contributions linked logically, and in an evidence-based way, to a particular
goal or goals for an individual. The emphasis of the NDIS is appropriately on the holistic
combination of supports that together provide support to meet the individual’s goals. So,
it is the cluster of supports which leads to achievement of a cluster of goals. Evaluating
the contribution of any one intervention is often difficult to disentangle.
110. I have raised the issue of holistic provision above, in the context of early intervention,
but the same issues apply to all aspects of the NDIS to a greater or lesser degree.
Unfortunately, the literature mostly only focuses on evaluating each therapeutic support
in isolation.
111. The third problematic element in the literature base is that the research evidence in
any field rarely says something is always beneficial or always not, rather, the critical
question is almost always how much and in what circumstances.
52 https://www.york.ac.uk/che/patient-outcome-tool/
53 Wallace, Jacqueline (2022), 'An Arts Therapists Guide to NDIS Therapy Report Writing', (North Brighton:
ANZACATA). The NDIA also provides guidance on reporting.
21
link to page 27 link to page 27
112. Phrased more formally, the key policy question is
in prospect, in what cases is art or
music therapy a reasonable and necessary therapeutic support as an alternative to art or
music activities. Possible factors may include, among others:
• Diagnoses and complexity (e.g., level of verbal communication)
• Treatment goals and outcomes (e.g., music activities are not a reasonable
alternative to some forms of therapy such as neurological music therapy)
• How much music therapy is reasonable and necessary in key scenarios.
113. As I have argued above, these factors can be assessed in prospect. For people like
the participant, is there rigorous evidence that art or music therapy might make a
difference in achieving their functional outcomes?
114. If art or music therapy were then added to the participant’s plan, progress might be
measured concurrently (or in retrospect). That is, given the specific circumstances of this
participant, working with this therapist, we see a trajectory of change from before the
support was provided until now, with reports to the NDIA being able to identify any
incremental benefit compared to the cost of the support.
115. Over time, the NDIA could use this data set to supplement the published literature to
identify, standardised for the type of participant, what expected trajectories might be, and
whether specific therapists are associated with better or worse trajectories for the
participant.
116. Public provision of provider- or team-specific information about impa
ct54 would assist
participants to choose amongst providers/teams, consistent with effecting the NDIS goal
about choice and control
.55
117. Returning to the question of ‘what is evidence?’, at minimum ‘evidence’ is about
systematic, controlled studies. By ‘controlled’ here I mean studies that compare the use
of art or music therapy with usual services, or with art or music activities not under the
guidance of an art or music therapist.
54 Information about names, locations and other attributes (e.g., languages spoken) of therapists is readily
available, but no information is provided about therapist quality.
55 The evidence about public provision of comparative quality data in health care is mixed; see Metcalfe,
D., et al. (2018), 'Impact of public release of performance data on the behaviour of healthcare consumers
and providers',
Cochrane Database of Systematic Reviews, (9). There may also be perverse effects, as
providers may distort data provision. That said, if choice and control is to be effected, it is important that
participants, carers and advocates are as fully informed as possible when selecting among potential
providers.
22
link to page 28 link to page 28 link to page 28 link to page 28 link to page 28
118. Although randomisation of groups to receiving or not receiving these supports or not
is ideal, other methods of control – such as case control studies – may yield comparable
information
.56 The point here is that there needs to be good evidence that the supports
achieve benefits in specific circumstances, in addition to reports of individual stories, for
a support to meet the threshold of ‘evidence based’ contemplated in the NDIS
definition
.57
119. A further weakness of the literature of the effectiveness of art and music therapy is
that the definition of art or music therapy used in the evaluations is often not as clear as
it could be, and so the conclusions from the literature are not always easily able to be
translated into policy. There are exceptions, of course, Hu et al.’s review of art therapy
has a table describing the treatment for each of the key articles reviewed
.58
120. Even when the interventions are well described, they might be quite heterogenous.
One systematic review noted that ‘the nature of music interventions … varied largely
across the studies
.’59
121. The Cochrane Review of music therapy in autism spectrum disorders described the
included studies thus:
The majority of studies included in this review examined music therapy in an
individual (i.e. one-to-one) setting (n = 13). In eight trials, music therapy was
delivered in a group setting. One study reported that music therapy was delivered
either individually or in small groups of up to three people, (another) applied a family-
based setting where parents or other family members were also involved in therapy
sessions. In four studies, it was unclear whether music therapy sessions were
conducted in an individual or group setting. The frequency of music therapy sessions
ranged from daily to weekly. In seven studies music therapy was provided daily, all
with a very short duration of one or two weeks. Of the studies that provided music
therapy over a longer time period, it was provided weekly in nine studies, twice
weekly in six studies, and in the remaining studies three, four, or six times per week.
One study randomised to either one or three session per week. The duration of
sessions ranged from 10 to 60 minutes with a median of 30 minut
es.60
56 Benson, Kjell and Hartz Arthur, J. 'A Comparison of Observational Studies and Randomized, Controlled
Trials',
New England Journal of Medicine, 342 (25), 1878-86.; Concato, John, Shah, Nirav, and Horwitz
Ralph, I. 'Randomized, Controlled Trials, Observational Studies, and the Hierarchy of Research Designs',
New England Journal of Medicine, 342 (25), 1887-92.; Pocock Stuart, J. and Elbourne Diana, R.
'Randomized Trials or Observational Tribulations?',
New England Journal of Medicine, 342 (25), 1907-09.
57 The NDIS Quality and Safeguards Commission discusses the concept of an evidence hierarchy in its
Evidence-Informed Practice Guide, see pages 4 +.
58 Hu, Jingxuan, et al. (2021), 'Art Therapy: A Complementary Treatment for Mental Disorders',
Frontiers in
Psychology, 12 (686006), 1-9.
59 Jordan, Catherine, Lawlor, Brian, and Loughrey, David (2022), 'A systematic review of music
interventions for the cognitive and behavioural symptoms of mild cognitive impairment (non-dementia)',
Journal of Psychiatric Research, 151, 382-90.
60 Geretsegger, Monika, et al. (2022), 'Music therapy for autistic people',
Cochrane Database of Systematic
Reviews, (5), CD004381. Page 21
23
link to page 29 link to page 29 link to page 29
122. Other reviews have made similar comments about the heterogeneity of what an art or
music therapy intervention might be. Ideally, as mentioned above, we should be able to
address the
how much question: we should be able to compare the effects of a one-on-
one intervention compared to a group session compared to no art or music therapy.
123. Similarly, it was often not clear what was the marginal benefit of an additional
session: should the therapy intervention be eight sessions with a therapist or ten? How
long should each session be to achieve the benefit?
124. Most importantly, there is also the question of who should provide each service?
125. There is an increasing expectation of health and disability professionals that they
should be able to work to their full scope of practice, using all the skil s and knowledge
they acquired in their professional training
.61 The corollary is that when those skil s are
not needed, the support/activity could be done by someone without those skil s and for a
lesser cost.
126. Specifically, should the role of the professional therapist be to design a program for
the person, with implementation the responsibility of the carer providing the support in an
integrated participant and carer-centred way? For example, the music therapist might
write a song which the parents sing and teach the participant to sing, to help with
undertaking hand washin
g62 or other everyday activities. The therapist might also train a
schoolteacher in appropriate techniques
.63 Or should the therapist delegate some of a
program to an assistant professional? In NDIS parlance, this might mean that the
therapist designs, and the next few sessions are art or music activities rather than art or
music therapy, with the therapist having another session later to monitor progress.
127. The reverse is also true: the art or music therapist might work with other therapists to
design an integrated multi-disciplinary program which the art or music therapist
implements on behalf of the whole team.
128. However, all this presupposes a truly multi-disciplinary way of working, easier in
organisational settings than in the home or a therapist’s rooms is in solo practice. As one
music therapist reflected to this review:
But we have lost the transdisciplinary ways of working that are often a signature of
organisation-based music therapy practice, particularly because music therapists can
61 Scope of Practice Review (Reviewer: Mark Cormack) (2024), 'Unleashing the Potential of our Health
Workforce: Final Report', (Canberra: The Review).
62 This is a real example provided in the submission from AMTA
63 Bentley, Laura A, et al. (2023), 'A translational application of music for preschool cognitive
development: RCT evidence for improved executive function, self‐regulation, and school readiness',
Developmental Science, 26 (5), e13358.
24
link to page 30 link to page 30 link to page 30
create motivating and rewarding conditions for people to rehearse and maintain skills
so we often support goals of our colleagues, as well as focusing on creative,
expressive, psychosocial emotional goals.
129. Final y, to what extent should art or music therapy be seen as time-limited, designed
to build capacity so that participants and their families/carers can use the techniques
they have learned (e.g., calming music) in an ongoing way without the presence of the
therapist?
130. Unfortunately, the published literature does not provide definitive answers to these
questions, pointing to a gap in the literature and a potential research agenda.
The quality of the literature
131. As evidenced in the submissions and from my own analysis, there is a growing
literature about the benefits of art and music thera
py,64 and a number of systematic
reviews. Systematic reviews and meta-analyses look across a number of studies, or
combine a number of studies, to get an overall picture of what is happening in a field and
can more precisely measure effect size. By combining studies one can be more certain
of their generalisability.
132. A systematic review generally assesses the quality of included studi
es.65 For both art
and music therapy, much of the literature is stil weak – poor quality designs, low
numbers – probably a sign that the fields are stil developing. A recent systematic review
of music therapy had this to say about the quality of the literature:
The literature had a number of limitations including small sample sizes, lack of
control group, lack of randomisation and lack of double blinding in (randomised
controlled trial) studies
.66
133. Nevertheless, despite these limitations, the overal pattern is that both art and music
therapy can make a meaningful difference in goal achievement for people with some
conditions.
64 Australian Music Therapy Association (2024), 'Music therapy Disability evidence summary 2024:
Person-first language', (Beaumaris, Vic: AMTA).
65 Grades of Recommendation, Assessment, Development, and Evaluation (GRADE) Working Group,
(2004), 'Grading quality of evidence and strength of recommendations',
BMJ, 328 (7454), 1490-94.;
Guyatt, Gordon H., et al. (2008), 'What is “quality of evidence” and why is it important to clinicians?',
BMJ, 336 (7651), 995-98.
66 Jordan, Catherine, Lawlor, Brian, and Loughrey, David (2022), 'A systematic review of music
interventions for the cognitive and behavioural symptoms of mild cognitive impairment (non-dementia)',
Journal of Psychiatric Research, 151, 382-90.
25
link to page 31 link to page 31 link to page 31 link to page 31 link to page 31
134. It is important to emphasise that not all systematic reviews are themselves of good
quality. Indeed, there are now tools to assess the quality of systematic reviews (e.g. risk
of bias)
.67
135. The literature essentially examines the
clinical benefit of the interventions, with
almost no studies of the
cost-effectiveness of the interventions
,68 whether increased
investment in the therapy would yield additional benefits, or whether reduced investment
could achieve the same benefit.
136. There was only one study of art therapy reported in the Tufts cost effectiveness
registry, and this related to non-psychotic mental health disorders
.69 This systematic
review cautioned about drawing definitive conclusions, given the heterogeneity of the
studies, risk of bias, and generally poor quality.
137. ANZACATA also drew my attention to an economic impact study about art therap
y.70
138. The Tufts cost effectiveness registry included only two studies related to music,
neither directly related to music therapy with people with disabiliti
es.71 Neither study
allows one to make definitive conclusions about the cost effectiveness of music therapy
for people with disabilities generally.
139. This paucity of evidence about cost-effectiveness of both modalities is unfortunate to
the say the least, and the NDIA might consider commissioning research to address this
gap.
67 Shea, Beverley J., et al. (2017), 'AMSTAR 2: a critical appraisal tool for systematic reviews that include
randomised or non-randomised studies of healthcare interventions, or both',
BMJ, 358 (j4008), 1-9.
68 The Tufts cost-effectiveness registry is the accepted registry of such studies: Thorat, Teja, Cangelosi,
Michael, and Neumann, Peter J. (2012), 'Skills of the Trade: The Tufts Cost-Effectiveness Analysis
Registry',
Journal of Benefit-Cost Analysis, 3 (1), 1-9.
69 Uttley, Lesley, et al. (2015), 'The clinical and cost effectiveness of group art therapy for people with non-
psychotic mental health disorders: a systematic review and cost-effectiveness analysis',
BMC Psychiatry, 15 (151), 1-13.
70 Bowen, Henry, et al. (2024), 'Social value of culturally informed art therapy for military and emergency
services',
International Journal of Art Therapy, 29 (4), 205-14.
71 One on community singing with older people (Coulton, Simon, et al. (2015), 'Effectiveness and cost-
effectiveness of community singing on mental health-related quality of life of older people: randomised
controlled trial',
British Journal of Psychiatry, 207 (3), 250-5.) and one on sound therapy for tinnitus
(Newman, Craig W. and Sandridge, Sharon A. (2012), 'A comparison of benefit and economic value
between two sound therapy tinnitus management options',
Journal of the American Academy of
Audiology, 23 (2), 126-38.)
26
link to page 32 link to page 32 link to page 32 link to page 32
140. Another weakness of the literature is often the effect demonstrated is quite small, so
although the result in the initial trial, or as revealed in a meta-analysis, is
statistical y
significant, it may make no real difference to a person in their everyday life.; The
concept of the ‘
minimal clinically important difference’,72 has been developed in the wider
literature to address this issue and better studies are beginning to discuss this.
141. Although there are stil methodological issues about identifying what is a clinically
important difference
,73 the concept is an important one, especially in the context of public
funding and in the absence of reliable cost effectiveness measures.
142. Inclusion in a plan of supports which do not meet a threshold of a clinically important
difference also comes at an opportunity cost, that is including this support may mean
another support which might make a bigger difference is not included in a participant’s
plan. There are wider opportunity cost issues too, as including a support which does not
reach a minimal threshold means the therapist time spent on that is not available for
other participants, and there is a cost to the public as wel .
It is recommended that the
new Evidence Advisory Committee considers the concept of a minimal clinically
important difference in making its recommendations.
143. The concept of the minimal clinically important difference also raises issues of
measurement error and reproducibility
.74 So for an individual, any measurement of their
functioning or outcomes has an inherent measurement error – and this is why most
clinicians will measure multiple times, to minimise the risk of treating ordinary variation
as being something of clinical importance.
144. The effect size found in many of the systematic reviews and meta-analyses is quite
small, but in some cases, it is quite reasonabl
e.75
145. Final y, the academic evidence relies on academics (and/or practitioners) having
time, funding, and an interest in researching an area. This results in gaps and
contradictions in the literature beyond methodological or study-design issues.
72 Hays, Ron D. and Woolley, J. Michael (2000), 'The Concept of Clinically Meaningful Difference in Health-
Related Quality-of-Life Research',
PharmacoEconomics, 18 (5), 419-23.
73 Mouelhi, Yosra, et al. (2020), 'How is the minimal clinically important difference established in health-
related quality of life instruments? Review of anchors and methods',
Health and Quality of Life Outcomes,
18 (136), 1-17.; Carrasco-Labra, Alonso, et al. (2021), 'Minimal important difference estimates for patient-
reported outcomes: A systematic survey',
Journal of Clinical Epidemiology, 133, 61-71.
74 Dvir, Zeevi (2015), 'Difference, significant difference and clinically meaningful difference: The meaning
of change in rehabilitation',
Journal of Exercise Rehabilitation, 11 (2), 67-73.
75 A good preprint review has a helpful table of effect sizes: de Witte, Martina, et al. (2025 (preprint)), 'The
Effects of Arts-Based Interventions in the Treatment and Management of Non-Communicable Diseases:
An Umbrella Review and Meta-Analyses',
Natureportfolio.
27
link to page 33 link to page 33 link to page 33 link to page 33 link to page 33
Where to from here?
146. Creative activities, in and of themselves, benefit all of us
,76 and there has been a
number of studies that identify physiological mechanisms and paths associated with
music
.77 The issue to be considered in this Review is the evidence base for a
therapeutic
intervention, compared to the ordinary life course with a person’s existing set of
interventions, and the relative benefit of therapy over
participation in art or music
activities.
147. As I have discussed above, there are many issues involved in weighing up evidence,
including what evidence to consider. I started this consideration of evidence citing a
definition of evidence-based practices as ‘practices for which there is a demonstrated
relation between specific practices and measured outcomes
.’78. Importantly and usefully,
the authors go on to clarify that
demonstrated relation here can be inferred if:
(a) there is substantial evidence that the outcome is caused by the practice, (b) it has
been demonstrated that the intervention clearly leads to the desired outcome, or (c)
there is a significant correlation between a specific practice and the measured
outcome (page 115).
148. This would be useful framing for the new Evidence Advisory Committee to adopt.
149. A recent very comprehensive ‘umbrella review and meta-analysis’ of arts-based
interventions in non-communicable disease was published as a preprint (that is, it has
not yet been peer reviewed)
.79 It included findings about mental health and neurological
conditions:
•
Mental health conditions We found a medium overall effect of arts-based
interventions on health outcomes in people with mental health conditions (0.53,
95% CI0.39–0.67, 78 ES, 30 SRs)
.80 Most ES were related to music (51 ES, 17
SRs), followed by mixed arts (7 ES, 2 SRs), visual arts (6 ES, 5 SRs),
drama/theatre (6 ES, 2 SRs), dance (4 ES, 4 SRs), and poetry/expressive writing
(4 ES, 11 3 SRs). The overall effect for psychological outcomes was medium. The
effect for physical outcomes was large but accompanied by a wide CI. We found
76 Daykin, Norma, et al. (2017), 'What works for wellbeing? A systematic review of wellbeing outcomes for
music and singing in adults',
Perspectives in Public Health, 138 (1), 39-46.
77 Fancourt, Daisy, Ockelford, Adam, and Belai, Abi (2014), 'The psychoneuroimmunological effects of
music: A systematic review and a new model',
Brain, Behavior, and Immunity, 36, 15-26. Sittler, Mareike
C., et al. (2021), 'Psychobiological mechanisms underlying the health-beneficial effects of music in
people living with dementia: A systematic review of the literature',
Physiology & Behavior, 233, 113338.
78 Schalock, Robert L., et al. (2017), 'Evidence and Evidence-Based Practices: Are We There Yet?',
Intellectual and Developmental Disabilities, 55 (2), 112-19. page 115
79 de Witte, Martina, et al. (2025 (preprint)), 'The Effects of Arts-Based Interventions in the Treatment and
Management of Non-Communicable Diseases: An Umbrella Review and Meta-Analyses',
Natureportfolio;
Finn, Saoirse and Fancourt, Daisy (2018), 'The biological impact of listening to music in clinical and
nonclinical settings: A systematic review', in Julia F. Christensen and Antoni Gomila (eds.),
Progress in
Brain Research (237: Elsevier), 173-200.
80 CI=Confidence interval; ES=Effect size; SR=Systematic review; QoL=Quality of life
28
a small effect for the QoL domain. The effect for cognitive functioning was
imprecise.
•
Neurological conditions: We identified a small-to-medium overall effect of arts-
based interventions for people with neurological conditions (0.40, 95% CI 0.30–
0.50, 276 ES, 67 SRs). Most eligible ES were related to dance (138 ES, 31 SRs),
followed by music (119 ES, 33 SRs), mixed arts (13 ES, 2 SRs), art (5 ES, 3
SRs), and drama/theatre (1 ES, 1 SR), with none for poetry/expressive writing.
The overall effect for physical outcomes was medium. Across the psychological,
cognitive, and QoL outcome domains, the effects were small.
150. As pointed out above, and as this latest preprint shows, the overall pattern in the
literature is quite variable.
The NDIA’s review of evidence
151. I was commissioned to consider ‘the NDIA’s ‘review of evidence’, which found that
there is limited evidence about the effectiveness of art and music therapy as evidence-
based’.
152. My view is that the conclusion explicit in my terms of reference, namely that there is
‘limited evidence’ about the effectiveness of art and music therapy is correct. It is also the
case that, for some conditions, there is insufficient evidence that art or music therapy
works to the extent necessary to meet any reasonable criterion for funding. But it is not
my view that limited evidence and no evidence are synonyms.
153. The NDIA’s evidence summary concluded:
This rapid review shows that there is some evidence which supports the use of art
and music therapy for certain disability groups (e.g. art therapy for children with
autism, music therapy for people with multiple sclerosis and people who have had a
stroke). Overall, the identified evidence was not conclusive in supporting art and
music therapy as evidence-based, therapeutic supports for all disability groups.
154. I agree with that conclusion.
155. The rapid review went on to conclude about art therapy that there was/were:
• Some evidence for the benefit of art therapy for children with autism across a
range of outcomes (mobility and movement, interpersonal interactions, and other
outcomes such as hyperactivity and inattention).
29
• Limited but positive indications for the benefit of art therapy across some
outcomes for adults with learning disabilities (on interpersonal interactions and
psychosocial functioning outcomes), children with cerebral palsy (on language
and communication outcomes), people with PTSD (on psychosocial functioning
outcomes), and people with anxiety and depression (on psychosocial functioning
outcomes).
• Limited evidence which indicated mixed and unclear benefit for people with
eating disorders and people with non-psychotic mental disorders.
• Limited evidence which indicated that art therapy may not provide any benefit for
children with learning disabilities and people with schizophrenia.
156. And with respect to music therapy the rapid review concluded that there was/were
• Some evidence for the benefit of music therapy for people with multiple sclerosis
and people who have had a stroke on mobility and movement outcomes.
• Limited but positive indications for the benefit of music therapy for people living
with Parkinson’s disease (on communication, mobility and movement and
psychosocial functioning outcomes), and people with depression and anxiety (on
interpersonal interactions and psychosocial functioning outcomes).
• Limited evidence which indicated mixed and unclear benefits for people with
autism, people with schizophrenia, people with PTSD, children with epilepsy, and
children with an intellectual disability and auditory processing disorder
157. There are three conclusions that one can draw from these findings. Firstly, one
cannot unequivocal y say that either art or music therapy are always beneficial for every
person. Secondly, nor can one say that art or music therapy are not effective for anyone.
158. Thirdly, and more importantly, the conclusions are nuanced. That is, for both art and
music therapy, the benefits are contingent; both art and music therapy have been shown
to be effective and beneficial for some conditions and for some functional outcomes. In
summary, the literature shows that effectiveness occurs at the intersection of the
condition and the functional outcome.
159. The NDIA’s rapid review summarises the literature using an example of what I would
call a matrix to show the condition-outcome pairs where art or music therapy are
effective.
160. Taking the evidence that I have reviewed, the submissions from stakeholders and the
NDIA’s own rapid review into account, the
key finding of this Review is that the
literature provides evidence that art and music therapy are effective and beneficial
to people in some circumstances, for example where the person has a specific
condition and where the therapy is relevant to their seeking to achieve a specific
objective or outcome.
161. It is a corollary of this that not every intervention provided by an art or music therapist
wil necessarily be of benefit to a particular participant.
It is recommended that the
NDIA, in messaging about evidence, should emphasise the benefits to a cohort of
30
link to page 36 link to page 36 link to page 36
participants receiving an art or music therapy intervention, distinguishing that
from generic advice about any intervention provided by art or music therapists.
162. It is beyond the scope of this review and inconsistent with the timelines I was given to
specify precisely what combination of conditions or diagnoses and for what functional
limitations is the literature sufficiently strong to demonstrate effectiveness.
It is
recommended that the new NDIS Evidence Advisory Committee should include an
assessment of the evidence base for art and music therapy interventions in
specific cohorts in its 2025-26 work plan. This assessment should focus on identifying
the goals and cohorts and dosage for which art or music therapy is likely to be more
valuable than only participation in art and music as an activity.
163. Information in plain language should be provided, possibly in a table/matrix showing
in what circumstances the literature shows a benefit should be produced and placed in
the public domain. The table should only include studies which demonstrate a minimally
clinically important difference. This should inform the plan approval process. That is,
therapeutic support should not be included in plans unless consistent with the evidence.
164. The evidence table should be supplemented by an interactive guide to help
participants, and their carers, advisors, and advocates, to identify what therapeutic
supports are likely to benefit them to achieve their goals, given their conditions.
165. Assessment of evidence – and development of evidence-based guidelines – is a
non-trivial task
,81 especially in the context of some groups being historical y excluded
from being participants in research studies. As the Deafblind Association argued:
gatekeeping the use of funds in this way risks participants from lesser understood
cohorts being denied effective supports on the basis that they have been historical y
excluded from academic research
.82
166. There is an old research adage that ‘absence of evidence is not evidence of
absence’. Accordingly, in considering guidance about the evidence base for small
cohorts, especially those who might have additional layers of disempowerment
,83 weaker
evidence should be considered for inclusion, and logical links accepted that this
81 Knaapen, Loes (2013), 'Being ‘evidence-based’ in the absence of evidence: The management of non-
evidence in guideline development',
Social Studies of Science, 43 (5), 681-706.
82 Deafblind Australia Submission to Independent Review of NDIS Art and Music Therapy Supports
83 Crenshaw, Kimberlé W (1989), 'Demarginalizing the Intersection of Race and Sex: A Black Feminist
Critique of Antidiscrimination Doctrine, Feminist Theory and Antiracist Politics',
University of Chicago
Legal Forum, 1989 (8), 139-67.; evidence-based decision making needs to incorporate equity issues
more: Hirsch, Bomi Kim, et al. (2025), 'Centering Equity in Evidence-Informed Decision Making:
Theoretical and Practical Considerations',
The Milbank Quarterly, 103 (1), 11-31.
31
link to page 37 link to page 37 link to page 37
therapeutic support works with this group, therefore, even though there is no published
evidence, it seems reasonable that it might work with another group.
167. In other settings, processes have been developed to support funding of an
intervention while the evidence is being developed, perhaps even from the cohort being
funde
d.84 The recent review of methods for health technology assessment in Australia
made a number of recommendations about strengthening the use of ‘real world
evidence’
.85
168.
I recommend that the new NDIS Expert Advisory Committee develop explicit
processes for making decisions about provision of therapeutic support in
populations where there is a poorly developed evidence base.
169. As the Royal Commission into Violence, Abuse, Neglect, and Exploitation of People
with Disability showed, ‘First Nations peoples’ understanding of disability does not easily
align with Western concepts of disability
…’86 One consequence of this is that the Expert
Advisory Committee may have to develop very different processes for assessing
evidence relevant to provision of specific supports for First Nations Australians.
170. However, subject to the small cohort issue discussed above, providing therapeutic
support where there is no evidence base is, in my view, unethical.
171. Participation in therapy comes at a cost to the participant of their time, sometimes
also travel to meet the therapist, and in the opportunity cost of not doing something else.
Sometimes costs for the parent or carer can be added to these. Given therapists are in
limited supply, if one person sees an art or music therapist for a condition for which there
is no evidence base, it precludes another person seeing that therapist for a condition
where there is a positive evidence base, creating a net loss in potential benefits to the
community. There is also a cost to the public in paying the therapist.
84 Federici, Carlo, et al. (2021), 'Coverage with evidence development schemes for medical devices in
Europe: characteristics and challenges',
The European Journal of Health Economics, 22 (8), 1253-73.;
Stafinski, Tania, McCabe, Christopher J., and Menon, Devidas (2010), 'Funding the Unfundable',
PharmacoEconomics, 28 (2), 113-42.
85 Health Technology Assessment Policy and Methods Review (2024), 'Accelerating access to the best
medicines for Australian now and into the future. A review of Australia's health technology assessment
policies and methods for the Australian Government', (Canberra: Department of Health and Aged Care).
Chapter 7.
86 Royal Commission into Violence, Abuse, Neglect, and Exploitation of People with Disability (2023),
'Final Report. Volume 9: First Nations people with disability', (Sydney: The Royal Commission).\, page 34
32
link to page 38 link to page 38
172. I heard stories from participants’ families where music therapy was not beneficial. It is
not clear whether these were instances where the evidence base for music therapy is
weak.
173.
I recommend the NDIA strengthen its oversight of plans to ensure that all
therapeutic support approved - not only in art or music therapy - has a robust
evidence base. The NDIA should ensure that data collected by the NDIA is collated
and analysed to ensure that the therapeutic support provided actually achieves a
result for the condition for this participant with this provider. Such a data set could
also be used to build evidence where it is currently lacking.
174. An exception to the plan approval process being limited to where the evidence is
already existing should be made where the program involves research for which ethics
approval has been obtained, or for very small participant cohorts where research has not
been conducted. Such an exception would be on a time-limited basis while the research
is conducted.
175. Strengthening oversight of plans would be facilitated by systematising reporting.
176. I was privileged to receive a number of anonymised reports submitted to the NDIA
reporting on participant progress. These were all submitted as narrative reports, in line
with the broad guidance provided by the NDIA
.87 Al the reports included information
about treatments and about the participant’s progress on relevant metrics, but how they
did this varied significantly.
177. Preparation of narrative reports allows provision of rich and nuanced data about the
participant’s progress, but they are expensive for professionals to prepare. They are also
hard for the NDIA to collate, even with use of artificial intelligence, as there is often
inconsistency in what measures are included in reports and how interventions are
descri
bed.88 It wil be recalled that systematic reviews of the value of art or music therapy
bemoaned the heterogeneity of the interventions involved in the reviews, and how they
were described.
178. Both description of interventions and measures used should be standardised. Ideally
both would cover multiple therapies, perhaps in the case of interventions using the
87 https://www.ndis.gov.au/providers/working-provider/connecting-participants/reporting-and-
participant-plan-reviews
88 The use of ‘AI scribes’ is growing as part of reducing the cost of preparing clinical notes and reports, see
e.g., Tierney Aaron, A., et al. 'Ambient Artificial Intelligence Scribes to Alleviate the Burden of Clinical
Documentation',
NEJM Catalyst, 5 (3), CAT.23.0404. AI scribes can allow user-specific formatting, and
this might be developed for NDIA reporting.
33
link to page 39 link to page 39 link to page 39 link to page 39 link to page 39 link to page 39 link to page 39 link to page 39
relatively new Rehabilitation Treatment Specification System
.89 Generic outcome
measures, such as the Australian Therapy Outcome Measures (Aus-TOMs)
,90 or the EQ-
5D91 might form the basis for reporting across a range of types of supports. The latter is
an interval-level measure and is widely used in economic evaluation.
179. The World Health Organization has supported the development of another measure
based on the International Classification of Functioning
,92 the World Health Organization
Disability Assessment Schedule 2.0
,93 and this is also used widely
.94 Therapy- or
diagnosis-specific tools might be used as an alternative or in addition to generic
measures, but these have variable psychometric properti
es.95
180. Systematising description and collection of both interventions and outcomes could
lead to a major reduction in the time taken by providers to provide data on treatments
and their outcomes and also improve efficiency within the NDIA. It wil also help, in the
longer term, to address one of the problems of developing appropriate payment design
.96
89 Van Stan, Jarrad H., et al. (2023), 'Rehabilitation Treatment Specification System: Identifying Barriers,
Facilitators, and Strategies for Implementation in Research, Education, and Clinical Care',
Archives of
Physical Medicine and Rehabilitation, 104 (4), 562-68.; Van Stan, Jarrad H., et al. (2021), 'Rehabilitation
Treatment Specification System: Methodology to Identify and Describe Unique Targets and Ingredients',
Archives of Physical Medicine and Rehabilitation, 102 (3), 521-31.; Zanca, Jeanne M., et al. (2019),
'Advancing Rehabilitation Practice Through Improved Specification of Interventions',
Archives of Physical
Medicine and Rehabilitation, 100 (1), 164-71.
90 Morris, M., et al. (2005), 'Reliability of the Australian Therapy Outcome Measures for quantifying
disability and health',
International Journal of Therapy & Rehabilitation, 12 (8), 340-46.; .; Perry, Angela, et
al. (2004), 'Therapy outcome measures for allied health practitioners in Australia: the AusTOMs',
International Journal of Quality in Health Care, 16 (4), 285-91.; Unsworth, Carolyn A., et al. (2004), 'Validity
of the AusTOM scales: A comparison of the AusTOMs and EuroQol-5D',
Health and Quality of Life
Outcomes, 2 (64), 1-12.
91 Feng, You-Shan, et al. (2021), 'Psychometric properties of the EQ-5D-5L: a systematic review of the
literature',
Quality of Life Research, 30 (3), 647-73.
92 World Health Organization (2001),
International classification of functioning, disability and health (Geneva: WHO).; although one should acknowledge critiques of the ICF: Imrie, Rob (2004), 'Demystifying
disability: a review of the International Classification of Functioning, Disability and Health',
Sociology of
Health & Illness, 26 (3), 287-305.
93 Üstün, T Bedirhan, et al. (2010), 'Developing the World Health Organization disability assessment
schedule 2.0',
Bulletin of the World Health Organization, 88, 815-23.
94 Federici, Stefano, et al. (2017), 'World Health Organization disability assessment schedule 2.0: An
international systematic review',
Disability and Rehabilitation, 39 (23), 2347-80.
95 Kumar, Mrityunjai, et al. (2024), 'Outcome Measures in intellectual disability: A Review and narrative
synthesis of validated instruments',
International Journal of Social Psychiatry, 71 (2), 239-53
96 Chalkley, Martin and Malcomson, James M. (2000), 'Government purchasing of health services', in
Anthony. J. Culyer and Joseph P. Newhouse (eds.),
Handbook of health economics: Volume 1A (Amsterdam: Elsevier), 847-90.
34
181.
I recommend that the NDIA systematise its collection of data from providers
about the effectiveness and outcomes of therapy interventions for participants,
including development of consistent definitions of interventions aligned to a
robust participant outcomes framework.
35
link to page 41 link to page 41
Pricing and rate setting
182. My terms of reference listed pricing first and the evidence base second, I have
reversed the order in this report as price is only relevant for evidence-based services.
That is, a therapy support should not be paid for if it is not likely to achieve a clinically
important outcome for participants.
183. In this section I use the term ‘payment rate’ to describe what is paid to providers
under the NDIS; generally, I reserve the term ‘price’ for market interactions
.97
184. Ideally, the payment rate for art and music therapy would reflect the value to the user
of the service. This would mirror the approach in an ordinary unregulated market, where
the consumer is wil ing to pay what they think the product is worth to them
.98
185. In the NDIS, the price to the recipient of the service is zero, that, is the full payment
for the service is made by the NDIA (or the self-managed participant) to the provider.
186. However, in most circumstances, a recipient’s NDIS allocation is essentially fungible,
that is, if money is not spent on one therapeutic support, it is available to be spent on
another. This means there is an ‘opportunity cost’ to the person with disability: what they
spend on art or music therapy is not available to be spent on something else. This is the
case for all participants irrespective of how their plans are managed, but it is
transparently so for self-managed participants.
187. But even so, apart from self-managed participants, the recipient does not completely
determine what is paid to the provider, as the payment is covered by the NDIS’
Pricing
Arrangements and Price Limits (PAPL).
188. The PAPL sets a payment rate maximum, and providers can charge less than that.
The PAPL describes ‘pricing’ thus:
• The NDIA does not set the prices that providers charge participants. Each
provider must agree the price for each support with each participant, subject to
the price limits and pricing arrangements that are imposed by the NDIA.
• Providers should not indicate in any way to participants that the prices that they
charge are set by the NDIA.
• In general, providers should not charge NDIS participants more for a support than
they would charge anyone else for the same support. If the price a provider offers
to a NDIS participant is different to that which they would offer to a person who
was not an NDIS participant, then the provider should ensure that the participant
is aware of this difference and the reasons for the difference (page 9).
97 I acknowledge that ‘administrative pricing’ is occasionally used in the literature.
98 The actual price paid in an unregulated market is determined by the intersection of what the consumer
is willing to pay and what price the provider/sel er is willing to sell for.
36
link to page 42 link to page 42 link to page 42
189. In effect, then, the NDIS oversees payment rates and, through the PAPL, sets a
maximum rate. This is essentially what I have been asked to review.
190. Because the payment for art and music therapy is made by the NDIS, and there is no
out-of-pocket cost to the participant, there is no effective market in that consumers are
not asked to make an individual valuation of what the service is worth to them and pay
accordingly.
191. In these circumstances, payment rates should reflect average benefit to the average
consumer
.99
192. Technically, payment should reflect the marginal benefit, and in the longer term, with
standardised information collected from providers, it wil be possible to track incremental
improvements and calculate the average of those incremental benefits to inform payment
policy.
193. There is extensive theoretical literature about measuring benefits, and so, if data
were available, it would be possible to set a fair payment rate relative to the average
benefit achieved. However, although the literature on measuring benefits is
longstanding
,100 it is stil controversial in the disability fiel
d.101
194. As I have concluded earlier, there is evidence that art and music therapy work in
certain circumstances, but the literature does not adduce estimates of the incremental or
average benefit of the proven interventions to be used in price setting.
195. Accordingly, setting aside the controversy about measurement, there is no reliable
data to set a payment rate based on average (or marginal) benefit.
196. The NDIS approach to setting rates or what is sometimes referred to as prices, is to
set rate maxima. The PAPL sets the following rate maxima:
99 Newhouse provides a useful review of pricing issues in health care, many of which are relevant to
disability services: Newhouse, Joseph P. (2002),
Pricing the priceless. A health care conundrum (Cambridge, Massachusetts: MIT Press).
100 Chen, Ariel, et al. (2015), 'The evolution of the disability-adjusted life year (DALY)',
Socio-Economic
Planning Sciences, 49 (March), 10-15.
101 Andrade, Gabriel (2024), 'Quality-Adjusted Life Years and Disability', in Gabriel Bennett and Emma
Goodall (eds.),
The Palgrave Encyclopedia of Disability (Cham: Springer), 1-8.
37
link to page 43
Table 2: Current rate maxima for selected services, per hour
Item Number
Item Name and Notes
Maximum
rate
15_610_0128_1_3
Assessment Recommendation Therapy or Training - Art
$193.99
Therapist
15_615_0128_1_3
Assessment Recommendation Therapy or Training - Music
$193.99
Therapist
15_054_0128_1_3
Assessment Recommendation Therapy or Training -
$222.99
Psychologist
15_056_0128_1_3
Assessment Recommendation Therapy or Training - Other
$193.99
Professional
043_0128_1_3
Assessment Recommendation Therapy or Training - Counsel or
$156.16
15_052_0128_1_3
Therapy Assistant - Level 1
$56.16
Support must be delivered by a therapy assistant working under
the delegation and direct supervision at al times of a therapist.
15_053_0128_1_3
Therapy Assistant - Level 2
$86.79
Support must be delivered by a therapy assistant working under
the delegation and supervision of a therapist, where the therapist
is satisfied that the therapy assistant is able to work
independently without direct supervision at al times.
Note: Rate maxima shown are for NSW, Victoria, Queensland and ACT, non-rural, non-remote. Other
areas have higher maxima.
197. The maximum payment rate for art and music therapists in the current PAPL (2023-
24) is the same as that for nationally regulated professions such as speech and
occupational therapy, below that for psychologists, and above that for counsellors, who
are not nationally regulated. Maximum rates for therapy supports, other than psychology,
have not increased since 2019 as until recently most claims were at rates below the
maximum.
198. Although the PAPL makes clear that the specified rates are the maximum that the
NDIS wil pay, there is no incentive on a provider to charge under the cap, or on
participants to see a provider who charges under the maximum
.102
102 Theoretically, the participant has a financial allocation, and they should have an incentive to shop
around to get best value for money. However, they can also ask for their allocation to be reviewed and
increased if it is fully expended which somewhat mitigates the incentive.
38
link to page 44
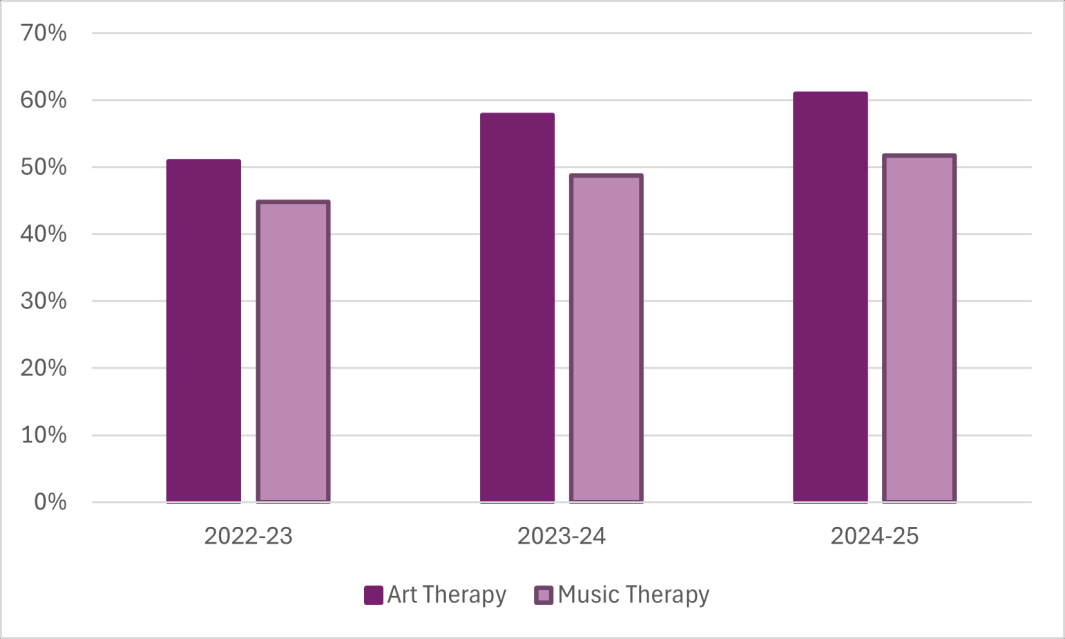
199. Further, the preconditions for effective market functioning are not present – not least
because of poor information about quality of different providers and consumers can only
judge the quality for them after they have experienced the servi
ce.103
200. As wil be shown below, in 2023-24 the rate maxima for both art and music therapy
appear to be above the prevailing rates in the outside market.
201. Setting rate maxima has serious limitations and risks.
202. Firstly, as mentioned above, there is effectively no incentive on providers to charge
less than the rate maxima. The PAPL specifies that
‘In general, providers should not charge NDIS participants more for a support than
they would charge anyone else for the same support’.
203. I have seen no evidence that any provider has been called to account for breaching
that specification, despite years of statistical evidence that this is a regular occurrence.
204. Secondly, there is no effective market in art or music therapy within the NDIS, and so
there is real y no ability of participants or their support people to look to price
competition, nor is there any real incentive to do so.
205. It is therefore no surprise that actual payments to art and music therapists are
tending toward the regulated maximum: more than half of all claims for art and music
therapy are now at or near the rate maxima (see Figure 1).
Figure 1: Proportion of payments at or near hourly rate maxima
103 Nelson, Phillip (1970), 'Information and consumer behavior',
Journal of political economy, 78 (2), 311-
29.
39
link to page 45
Data table for Figure 1
Art Therapy
Music Therapy
2022-23
51%
45%
2023-24
58%
49%
2024-25
61%
52%
Source: NDIA analysis, ‘at or near’ defined as $190-195
206. Thirdly, NDIS rates appear to be influencing the wider market, to the extent there is
one. That is, prices charged in the wider market appear to be drifting up to the NDIS rate
maxima.
207. Art and music therapy are very small professions and, as the NDIS has grown, it has
become the main purchaser of non-salaried art and music therapy. Effectively, the NDIA
is becoming a monopsonistic purchaser in these fields
.104
208. It has been argued that art and music therapists should have the same maximum
rate as physiotherapists, occupational therapists or speech therapists, essential y
because the training programs are somewhat similar. Indeed, my terms of reference
directed me to look at the rate maxima for other allied health professions. But there are
differences between the professions as wel , most notably that art and music therapy are
not nationally regulated.
209. The argument for parity is predicated on the assumption that the payment rate for the
chosen comparator is fair, and there is parity in all respects. However, in the short time
available for this review I cannot determine whether the maximum payment rates for the
other therapies are fair or not.
104 A monopsony is the buyer side parallel to a monopoly: a monopoly exists when there is a single seller
or provider, a monopoly exists when there is a single buyer or purchaser. Robinson, Joan (1969),
The
economics of imperfect competition (New York, NY: St Martins Press).; Thornton, Robert J. (2004),
'Retrospectives: How Joan Robinson and B. L. Hallward Named Monopsony',
Journal of Economic
Perspectives, 18 (2), 257-61.
40
210. But I wil go this far, as I have argued above there is good evidence that art and
music therapy can make a real difference for participants. Further, the evidence shows
that art and music therapy make a difference in some circumstances over and above
participation in art and music activities. The corollary of this is that art and music therapy
should continue to be paid as therapy rather than as participation in activities. This of
course leaves open the question about where precisely that professional rate should be
set.
211. Another way of phrasing this is to say that if art or music therapy is included in a
participant’s plan as an evidence-based stated support, then it should be paid as such,
as a therapy, else it should be paid as a participation activity.
212. My assumption here is that art or music therapy are included in a participant’s plan
as therapeutic supports because the aim is for the therapy to have a clear and defined
benefit linked to the participant’s needs. As I have said, it should then be paid as a
therapy.
213. Participant’s may want to accrue other benefits from involvement in art or music: to
calm, to engage with others, or generally to benefit as we all do from these activities.
These engagements should be paid for as participation in activities, not as therapy.
214.
I recommend that the NDIA set rate maxima for art and music therapists on the
basis that these are distinct professions, providing evidence-based therapy, not
simply supervising art or music activities.
215. As indicated above, in a normal market, a person assesses what the value of the
service is to them and is wil ing to pay commensurately. Importantly, art and music
therapists provide services outside the NDIS and so another comparator is how do other
users value art and music therapy?
216. Although there are good reasons to compare the prices that users outside the NDIS
are prepared to pay for art and music therapy, it is not a perfect comparison, as services
provided outside the NDIS may be slightly different from the services provided to people
eligible to receive NDIS support. Nevertheless, prices in an ordinary market may provide
a useful benchmark in relation to NDIS benchmarks.
217. As part of its annual pricing review, the NDIA analyses what private therapists charge
outside the NDIS as reported on their websites. The results for art and music therapists
for 2023-24 and all therapists are shown in Table 3.
41
Table 3: Summary Statistics of Private Billing Rate Sample, by Therapy Type, 2023-24
NDIS
Type of
Standard
25th
75th
Count
Mean
Min
Median
Max
price
Therapy
Deviation
percentile
percentile
limit
Art Therapy
26 $154.5
$30.6
$100.0
$135.0
$147.5
$178.8 $216.0
$193.99
Music
39 $166.0
$36.7
$90.4
$120.0
$180.8
$194.0 $233.3
$193.99
Therapy
All therapy
1,791 $195.6
$56.0
$85.0
$158.0
$194.0
$230.0 $396.0
Varies
supports
Source: 2023-24 Annual Pricing Review Report, page 79
218. On average (mean), a session of art therapy in 2023-24 cost a person outside the
NDIS about $40 below the NDIS payment maximum (median: about $45 below). The
price for music therapy outside the NDIS was also on average about $30 below the NDIS
maximum rate (median about $15 below NDIS maximum). That is, market prices for art
therapy were on average 80% of NDIS price caps, and for music therapy, 86% of the
maximum NDIS rate.
219. I have used the average market price here as the comparator. If one took a tighter
standard, say the 25th percentile there is an even bigger disparity between charges to
private clients and the NDIS. However given the NDIS’s monopsonistic positioning, the
mean seems reasonable for the purposes of these comparisons.
220. Although there may be differences between therapy services provided to NDIS and
non-NDIS clients, and the reporting associated with service provision, the magnitude of
the payment differences seen in 2023-24 is hard to explain, other than the effect of NDIS
maximum rate setting.
221. My conclusion is the NDIS maximum rate for both art and music therapy for 2023-24
was too high and potentially facilitated faster rate increases than was warranted e.g.,
relative to inflation. A fairer rate maximum for both art and music therapy would have
been the rate maximum for counsel ors.
222. Figure 2 shows that average prices charged outside the NDIS have drifted up to the
NDIS maximum rate over the last four years. The 10%-12% cumulative annual growth
rate (CAGR) seen is well in excess of the effect of inflation: the Consumer Price Index
showed a 3.5% cumulative annual growth rate over this period.
42
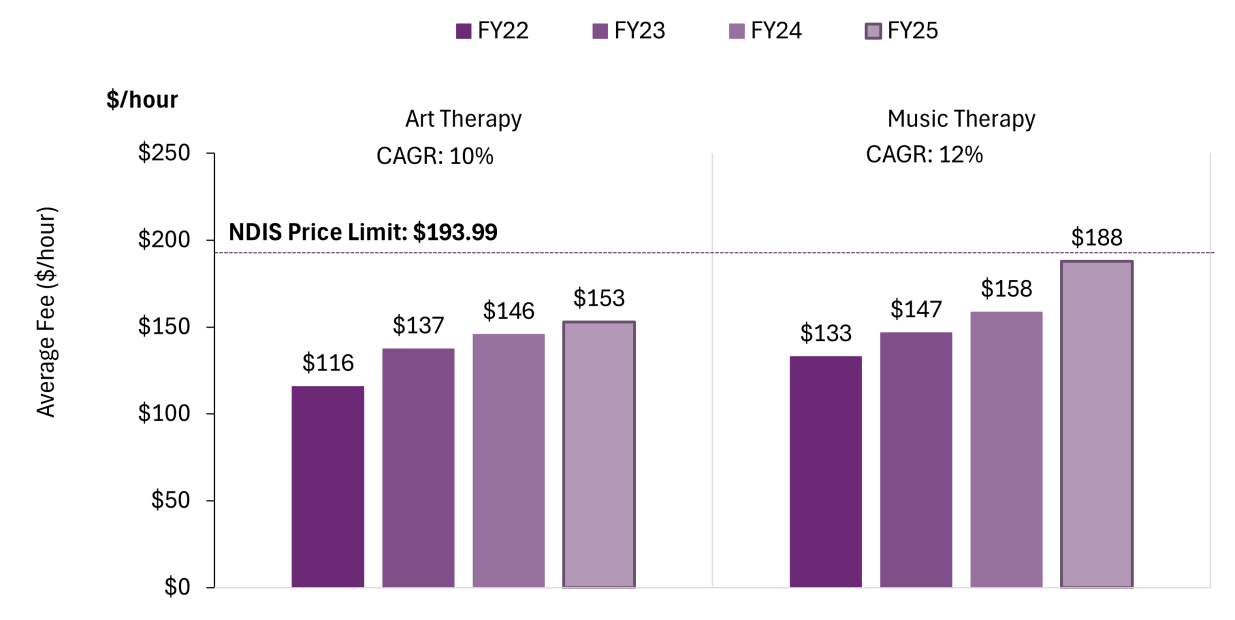 Figure 2: Average charge to clients outside the NDIS, recent years
Data table for Figure 2
Figure 2: Average charge to clients outside the NDIS, recent years
Data table for Figure 2
FY22
FY23
FY24
FY25
Art Therapy
$116
$137
$146
$153
Music Therapy
$133
$147
$158
$188
Source: NDIA, website scraping data
223. The shift in prevailing payment rates from 2023-24 to the present shows that the
NDIS rate maximum is an asymptote for prevailing prices. Importantly this is the case
both for NDIS services and for services provided outside the NDIS.
224. This il ustrates my earlier point about NDIA market dominance: that the NDIA has
essential y become a monopsonistic purchaser, setting prices for both NDIS services and
for services outside the NDIA's purview.
225. The NDIA payment rate has therefore become the pricing benchmark for all other
services, such as public community and mental health services. To the extent that
salaries of art and music therapists employed in these settings have not kept pace with
movements in the effective payment rate under the NDIS, the high NDIA payment rate
leads to a ‘crowding out’ effect. This means that other public services may not be
competitive in attracting art or music therapists and so art and music therapy become
less available in these other settings. This may lead to an overall reduction in societal
utility, as people not covered by the NDIS can no longer get access to evidence-based
art or music therapy.
43
link to page 49
226. Another effect of the NDIA’s dominant role in the broader rate/price setting for art and
music therapy is that looking to the private market for benchmarking is somewhat circular
- the NDIA rate setting affects those prices as well.
227. How then might the NDIA set rate maxima? The simple answer is what is best for
participants and the public. Ideally the payment rate should reflect marginal value, but we
don't have the evidence to do that.
228. The next best approach is for the NDIA to become a more sophisticated market
steward as contemplated in the NDIS Review
.105
229.
I recommend that the NDIA expand its capacity monitor market dynamics to
assess supply of, and the demand for, art and music therapy and therapists.
230. Demand for art and music therapists is dominated by the public sector, particularly
the NDIS, as most users of art and music therapy are NDIS participants. Other public
sector payers – such as state governments for mental health services – could easily be
captured in evaluations of demand.
231. Supply of art and music therapists is affected by entry and exits, the former
constrained by the number of approved education programs for these professions. The
NDIA or the Department of Social Services could foreshadow to educational providers its
estimates of future demand to assist them in planning the size of their intakes.
232. A potential constraint on supply is the availability of placements for art and music
therapy students. Although this was only raised with me in this Review in passing, the
issue of finding placements for students is a perennial one, exacerbated in professions
which are predominantly private, one: one provision, with fee-for-service remuneration,
all characteristics of art and music therapy. In the medium term, strategies may need to
be considered to facilitate or fund placements through additional payments to providers
of art or music therapy to supervise students on placement.
233. Another critical variable in estimating supply is the response of therapists to change
in payment rates: if the NDIA rate is too low, therapists might choose leisure or
alternative work rather than support NDIS participants. Assuming that all future NDIS
provision is evidence-based in line with my recommendations, a level of supply that is
less than the level of demand would involve a net loss in societal welfare.
105 Independent Review into the National Disability Insurance Scheme (2023), 'Final Report: Working
together to deliver the NDIS', (Canberra: The Review). The Department of Social Services already
undertakes demand mappin
g: https://caresectordemandmap.dss.gov.au/map/ndis/postcode
44
234. The objective of workforce analysis would be to ensure that there are sufficient art
and music therapists so that evidence-based art and music therapy is available to all
NDIS participants if it is included in their plans. Demand outside the NDIS also needs to
be considered. Any workforce analysis would also benefit by being segmented by
geography, to ensure access for people in rural and remote Australia.
235.
I recommend that in the medium term the NDIA, set payment limits for art and
music therapy that take account of their labour market monitoring and the need to
ensure there is an adequate supply of art and music therapists to meet the
requirement for evidence-based provision of art and music therapy.
236. But a payment rate maximum for each of the relevant professions needs to be set in
the meantime while the longer-term strategy is addressed.
237. Due to the circularity involved in the interaction between the NDIA rate maxima and
the private market, unfortunately there is no other basis for setting a rate maximum
currently.
238. I have seen no evidence that the increase in charges for art and music therapy seen
in the last few years is associated with improvements in outcomes. Rather, I think it is
simply the outworkings of the drift upwards in charging in the absence of an effective
market for these services.
239. Accordingly, I think the evidence about the relationship between NDIA rate maxima,
charges by therapists to the NDIA, and external market pricing, as shown in the
previously published NDIA market review should be the basis for rate maxima.
240. However, as recommended above, it is not my view that art or music therapy is
simply another form of art and music activity, so rate maxima for these services should
be aligned with professional, rather than participation in an activity, rates.
241. The previous NDIS pricing review showed that there was alignment in the
marketplace of the rate for both art and music therapy with the rate maximum for
counsel ors.
242.
I recommend that the NDIA align the maximum payment limit for art and music
therapy with the maximum payment limit for counsellors. To be explicit, this
recommendation applies to the separate rates established for early intervention services.
243. The PAPL schedule includes a rate maximum for ‘other professionals’. A potential risk
of this recommendation is that art and music therapists might use that item, which has a
higher maximum, rather than the existing art and or music therapy code which would
have a newer rate maximum. To avoid this perverse consequence,
I recommend that
45
the NDIA specify in its Pricing Arrangements and Price Limits, that art and music
therapy cannot be claimed under ‘other professional’.
244. The current PAPL sets a single payment rate for each class of allied health
professional, including art and music therapists, so a new graduate and a therapist with
years of experience can claim the same rate.
245. Patently, therapists might differ in their skil s based on their experience and further
study. One would typically expect to see a large variation in rates charged to the NDIA to
reflect this. We don't. Rather what we see as exhibited in Figure 1 more than half of
claimed rates are close to the rate maximum.
246. Overtime, it might also be useful to recognise specialisation and advanced skil s
within allied health professions, including art and music therapy. This would help to
ensure that the most skil ed therapists are appropriately remunerated for dealing with
participants with more complex needs.
247. The PAPL already provides for two rates for therapy assistants.
248.
I recommend that the NDIA explore establishing differentials within the allied
health professionals’ scales to recognise different capacity to provide services
and/or to recognise levels of skills and experience.
249. Payments by self-managed participants are not regulated by the PAPL. However,
self-managed participants can only spend under their plan budgets in line with NDIS
guidelines, that is, the therapeutic support provided must be evidence based.
250. Appropriately, self-managed participants have freedom to choose who provides
therapeutic support. This freedom is not unconstrained, as what is provided must be
consistent with the definition of therapeutic support. This suggests that the person
providing the therapeutic support should be appropriately qualified and understands what
evidence-based support is and what it is not.
251.
I recommend that the NDIA ensure that funding for art and music therapy as a
Therapeutic Support for self-managed participants be limited to supports provided
by appropriately trained art and music therapists as defined by NDIA who meet the
requirements of NDIS Commission registration. In other circumstances, art or
music activities should be classified as Participation in Community, Social and
Civic Activities and funded accordingly.
252. The provision of art and music therapy, and payment arrangements, reflect a
‘professional’ model of provision involving fee-for-service payment. Essentially, a
46
link to page 52
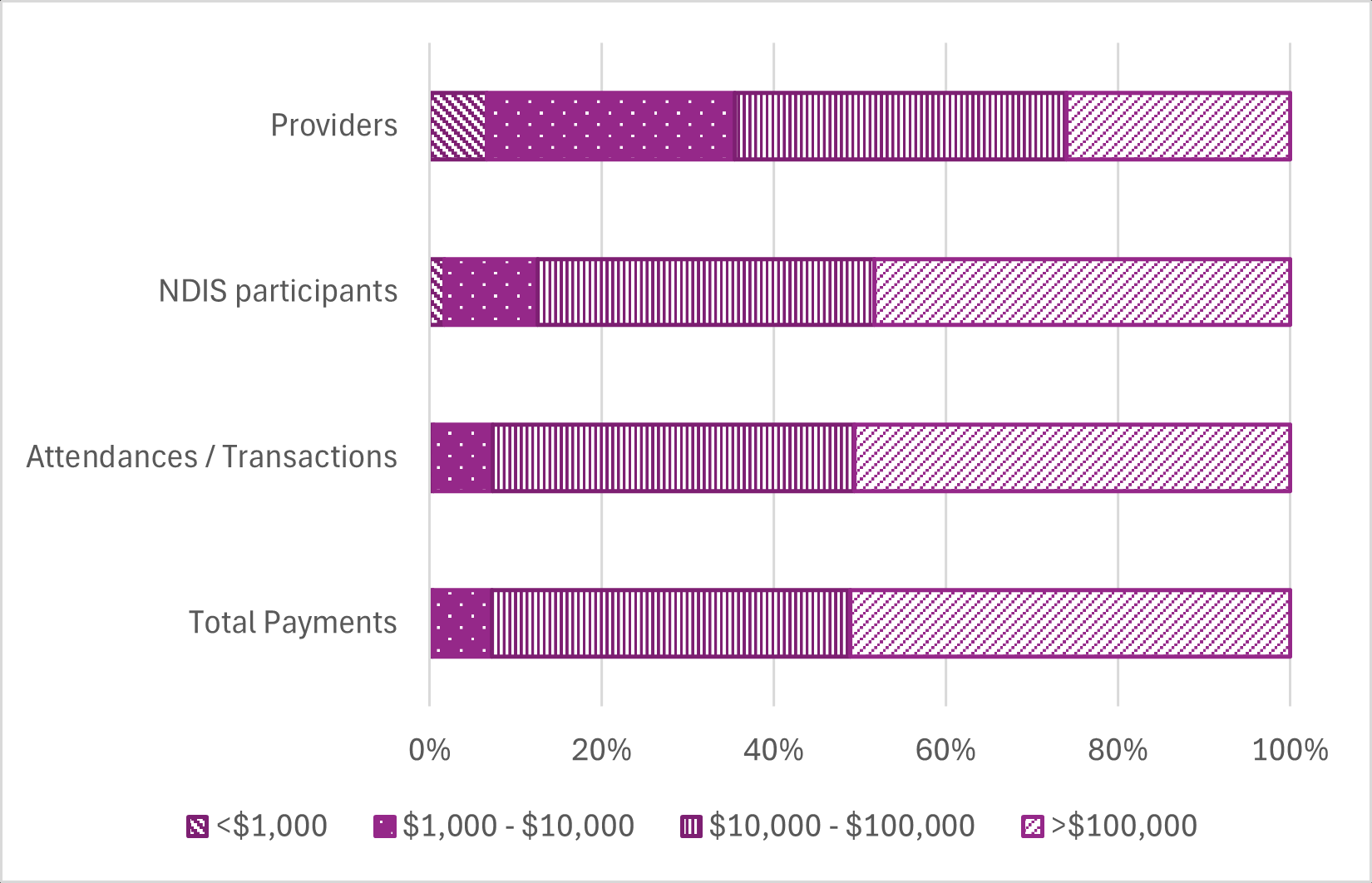
hal mark of professions is that expertise is institutionalised in an individual profession
,106
with payment between the professional and the client, typically paid as a fee-for-service.
Traditionally there were no third-party payers.
253. The NDIS is a third-party payer which potentially calls into question whether the
historic fee-for-service model continues to be fit-for-purpose.
254. Many art and music therapists see only a few NDIS clients and so the fee-for-service
model may continue to be appropriate here, but in both fields, there are large providers
with a quite different service model.
Figure 3: Provision of art therapy, by size of provider in terms of total NDIS payments,
2023-24
106 Abbott, Andrew (1988),
The system of professions: An essay on the division of expert labor (Chicago:
University of Chicago Press).
47
link to page 53 link to page 53
Data table for Figure 3
<$1,000
$1,000 -
$10,000 -
>$100,000
$10,000
$100,000
Total Payments
0.0443
0.92073
5.57791
6.83243
Attendances /
289
4714
28594
34515
Transactions
NDIS
121
754
2722
3367
participants
Providers
111
482
644
435
Source: NDIA, data provided to review. Note: Payments are total NDIS payment to the provider, not just for art
therapy. Providers could claim other therapies, or other NDIS supports (e.g., disability support workers), noting
that NDIS provider is not equivalent to the actual therapist who provided the service
255. About one quarter of providers who have claimed for art therapy received more than
$100,000 of total NDIS revenue in 2023-24 (defined here as a large provider), but these
large providers have claimed almost half the art services (called
attendances/transactions in the figure) and received more than half the total art therapy
payments.
256. Compared to the smallest providers, the largest providers of art therapy:
• Received higher average payments per service ($198 v $152)
• Claimed more for each NDIS participant treated ($2029 v $364)
• Saw participants more frequently (average 10.3 services per participant v 2.4)
.107
257. The data provided to me does not enable me to assess whether participants seen by
the largest providers are more complex (so justifying some more visits), achieve better
outcomes (again potentially justifying more visits), or whether this simply reflects provider
and/or participant preferen
ces.108
107 I also looked at providers in the $1,000 - $10,000 range. They also saw participants less frequently (6.3
vs 10.3 for largest providers.
108 The economics literature refers to this concept as ‘moral hazard’, although the concept is under
challenge see Grignon, Michel, et al. (2018), 'Moral Hazard in Health Insurance',
Œconomia. History,
Methodology, Philosophy, (8-3), 367-405. Where the variation in use is driven by provider choices it is
referred to as supplier- or provider-induced demand. Various hypotheses have been advanced for the
phenomenon including income maximisation and professional uncertainty.
48
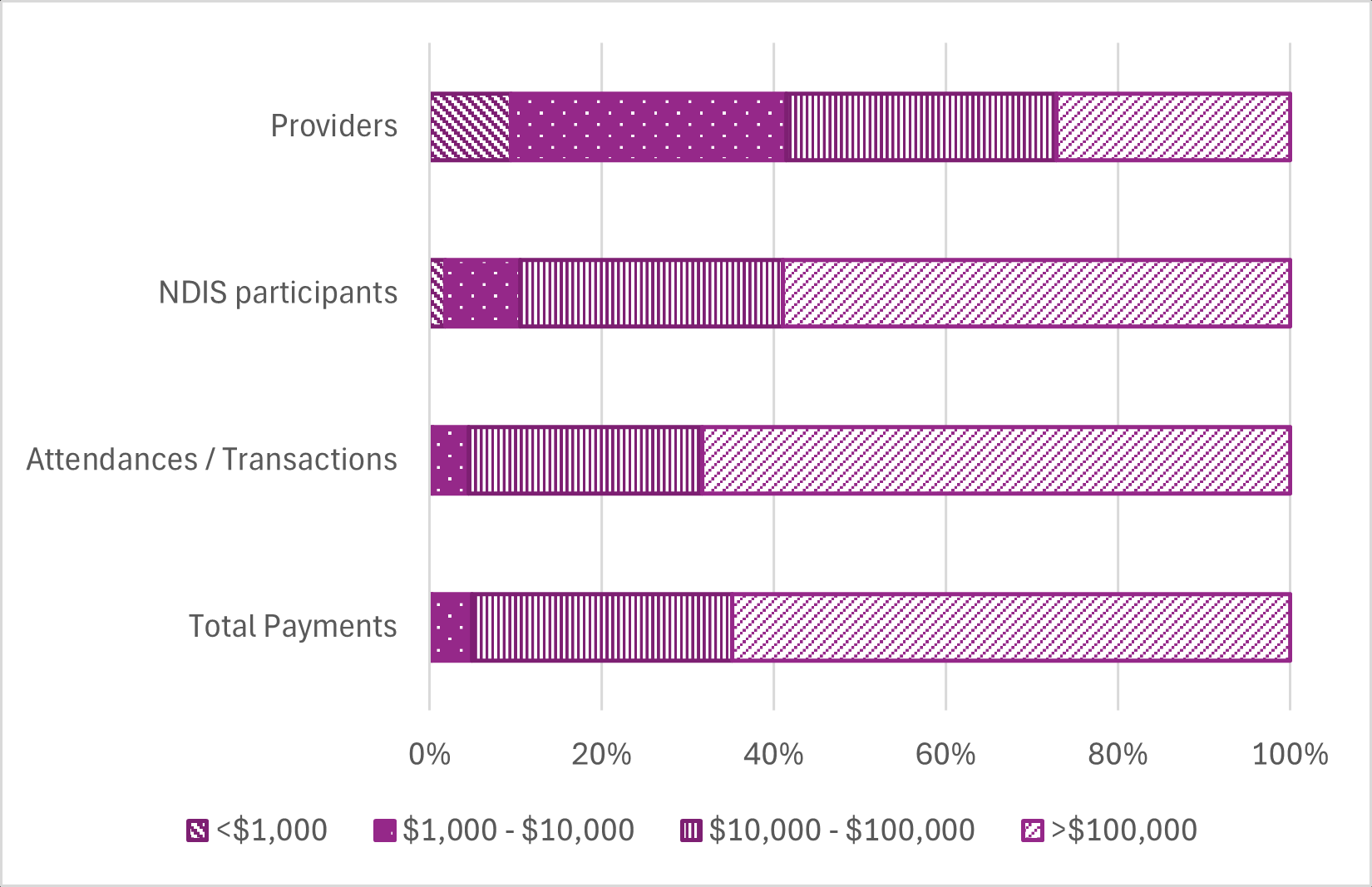 Figure 4: Provision of music therapy, by size of provider in terms of total NDIS
payments, 2023-24
Data table for Figure 4
Figure 4: Provision of music therapy, by size of provider in terms of total NDIS
payments, 2023-24
Data table for Figure 4
<$1,000
$1,000 -
$10,000 -
>$100,000
$10,000
$100,000
Total Payments
0.04714
0.74591
4.89062
10.4954
Attendances /
390
4550
29990
75498
Transactions
NDIS
133
640
2246
4331
participants
Providers
132
450
442
381
Source: NDIA, data provided to review. Note: Payments are total NDIS payment to the provider, not just for music
therapy. Providers could claim other therapies, or other NDIS supports (e.g., disability support workers), noting
that NDIS provider is not equivalent to the actual therapist who provided the service.
49
link to page 55 link to page 55
258. We see a similar pattern of claiming with music therapy providers. The largest
providers (those with total NDIS revenue in 2023-24 of more than $100,000) account for
just over one quarter of al providers who claimed music therapy, Similar to art therapy,
almost 60% of participants who received music therapy, used one of the largest
providers. The largest providers claimed for more than two thirds of the services and
received almost two thirds of the music therapy payments.
259. Compared to the smallest providers, the largest music providers:
• Received higher average payments per service ($139 v $121)
• Claimed more for each NDIS participant treated ($2423 v $353)
• Saw participants more frequently (average 17.4 services per participant v 2.9).
260. Again, we cannot make any definitive conclusions about the different practice
patterns.
261. The largest providers of both art and music therapy use company or trust structures
(79% of the largest art therapy providers and 85% of the largest music therapy providers
are companies or trusts) compared to the smaller providers who tend to be
unincorporated individuals or partnerships (85% of small art therapy providers and 95%
of small music therapy providers have adopted these structures).
262. Service provision by larger providers is different from the smaller providers and
warrants a different approach from the NDIA, including consideration of whether fee-for-
service is the best way of paying for their services
263. Normal business practice involves different bases for payment, including commercial
or relational contracts. Here, there may be elements of fee-for-service, but the contract
may be on a different basis more suitable to share benefits, say, of economies of scale
and to introduce payment models more appropriate for a regulated market
.109
264. In the case of art and music therapy, the NDIS might be able to articulate different
and/or greater expectations for the larger providers. For example, larger providers might
be expected to have a greater share of their provision in group work
;110 may have greater
expectations about training the next generations of therapists; or have greater
109 Laffont, Jean-Jacques and Tirole, Jean (1993),
A theory of incentives in procurement and regulation (Cambridge, MA: MIT Press).
110 It is important to note that group sessions are not appropriate for every participant: it may take time for
a participant to be comfortable in a group setting, or they might upset other people in the group. I also
heard stories of NDIS participants looking forward to group activities, building their skills there, and
learning how to make friends through participation in therapy sessions.
50
link to page 56 link to page 56
expectations about more sophisticated quality improvement practises; and better
measurement of the outcomes of their services.
265. The NDIA’s payment framework for these larger providers should consider the full
range of service benefits that are linked to participant needs over the short, medium and
long term. The framework should consider the most efficient and effective ways to set
payment limits for these services and the best payment arrangements that can ensure
their delivery.
266. Differential payment for larger providers has been canvassed previously, based in
part on arguments about different complexity of their clients, greater roles in workforce
development, and stronger mechanisms for quality improvement
.111
267. For larger providers, payment for training and research might be a supplement to
service provision payme
nts.112
268. As outlined in the discussion on early interventions services, client choice and control
would be maintained by their ability to ‘exit’ – their ability to move between providers
should not be constrained, perhaps with the exception of a specified notice period.
269. A key challenge in establishing a robust payment regime in the NDIS is the range of
cost structures and benefits delivered across a broad range of providers. Large providers
probably accrue all the benefits of economies of scale and other efficiencies, with no
explicit or apparent sharing of those benefits with participants or in improving NDIS
sustainability. What needs to be considered is how the NDIA might develop payment and
funding approaches that facilitate better collaboration among participants to extract value
from the larger providers.
270.
I recommended that the NDIA consider a different payment and funding
approach, particularly for large organisational providers.
111 Deloitte - Access Economics (2023), 'NDIS Therapy Pricing Structures – Options Analysis', (Canberra:
Deloitte - Access Economics).
112 In the health sector these services are recognised as distinct additional roles which need to be paid
for, with distinct additional payments not built into a higher payment cap for larger providers
51
Conclusion
271. It is clear from my review of the literature, that art or music therapy can be valuable
contributions to helping participants achieve their goals. But these therapeutic supports
are only likely to do this if there is good evidence to support this use of art or music
therapy from the experience of people with similar conditions and similar goals as
revealed in replicable research.
272. It is a waste of money to incorporate any therapeutic support in a plan in the absence
of good prospective evidence.
273. More information needs to be available to participants so that they are aware of what
works and what doesn't. Better information, and tighter linking of evidence and plans, wil
be helpful to both participants and the overall sustainability of the NDIS. I hope my
recommendations go some way to achieving this.
274. I would again like to thank all those who participated in this review, and those who
supported the review.
52
Document Outline