Research Team
Ciara Smyth, Trish Hill, Andrew Griffiths, Ilan Katz and Aran Mahenthirarajah
For further information:
Dr Ciara Smyth, x.xxxxx@xxxx.xxx.xx, 02 9385 7844
Social Policy Research Centre
UNSW Sydney 2052 Australia
t +61 (2) 9385 7800
f +61 (2) 9385 7838
xxxx@xxxx.xxx.xx
www.sprc.unsw.edu.au
© UNSW Sydney 2017
The Social Policy Research Centre is based in Arts & Social Sciences at UNSW
Sydney. This report is an output of the
Post Implementation Review of No Jab, No
Pay 2015 Budget measure research project, funded by the Australian Government
Department of Social Services.
Suggested citation:
[to follow] Smyth, C., Hill,T, Griffiths, A., Katz, I. and Mahenthiraraja, A. (2017).
Post
Implementation Review of the No Jab, No Pay 2015 Budget Measure (SPRC Report
09/17). Sydney: Social Policy Research Centre, UNSW Sydney.
Social Policy Research Centre 2017
ii
link to page 3 link to page 4 link to page 4 link to page 5 link to page 6 link to page 7 link to page 8 link to page 9 link to page 10 link to page 13 link to page 14 link to page 15 link to page 16 link to page 17 link to page 21 link to page 22 link to page 23 link to page 23 link to page 23 link to page 24 link to page 24 link to page 25 link to page 25 link to page 30 link to page 34 link to page 49 link to page 52 link to page 55 link to page 65 link to page 70 link to page 73 link to page 73 link to page 76 link to page 80 link to page 87 link to page 94
Contents
Contents .......................................................................................................... i
Tables ............................................................................................................ ii
Figures ........................................................................................................... ii
Glossary ......................................................................................................... iii
Executive summary ........................................................................................ 4
Policy design ........................................................................................... 5
Issues and risks ...................................................................................... 6
Communications ..................................................................................... 7
Management information ......................................................................... 8
1
Introduction ........................................................................................... 11
2
Literature review .................................................................................... 12
2.1 Immunisation rates .......................................................................... 13
2.2 Factors contributing to incomplete childhood immunisation ............ 14
2.3 Increasing immunisation uptake ...................................................... 15
2.4 The No Jab No Pay budget measure .............................................. 19
3
Methodology .......................................................................................... 20
3.1 Document review ............................................................................ 21
3.2 Data scoping ................................................................................... 21
3.3 Qualitative stakeholder consultation ................................................ 21
3.4 No Jab, No Pay workshop ............................................................... 22
3.5 Analysis and synthesis of findings ................................................... 22
4
Findings ................................................................................................. 23
4.1 Policy Design .................................................................................. 23
4.2 Implementation and Policy Design .................................................. 28
4.3 Dealing with issues and risks .......................................................... 32
4.4 Governance ..................................................................................... 47
4.5 Service delivery ............................................................................... 50
4.6 Communications ............................................................................. 53
4.7 Management information ................................................................. 63
5
Discussion ............................................................................................. 68
6
Impact Evaluation Framework ............................................................... 71
6.1 No Jab, No Pay theory of change ................................................... 71
6.2 No Jab No Pay Policy logic ............................................................. 74
6.3 Data Scoping ................................................................................... 78
6.4 No Jab, No Pay Impact Evaluation Framework ............................... 85
7
References ............................................................................................ 92
Social Policy Research Centre 2017
i
link to page 22 link to page 35 link to page 55 link to page 55 link to page 83 link to page 75 link to page 78
Tables
Table 1 Research areas, questions and data sources ................................. 20
Table 2 No Jab No Pay DSS risk log ............................................................ 33
Table 3 NJNP communication objectives, department responsible & target
audience ....................................................................................................... 53
Table 4 Data sources for impact evaluation ................................................. 81
Figures
Figure 1 No Jab No Pay Theory of change .................................................. 73
Figure 2: No Jab, No Pay Policy logic model................................................ 76
Social Policy Research Centre 2017
ii
Glossary
ACIR Australian Childhood Immunisation Register
AIR
Australian Immunisation Register
CCB Child Care Benefit
CCR Child Care Rebate
COs
Conscientious Objectors
DET
Department of Education and Training
DHS Department of Human Services
Health Department of Health
DSS
Department of Social Services
ES
External stakeholders
FTB
Family Tax Benefit
GS
Government stakeholders
NJNP No Jab, No Pay
VOs
Vaccination Objectors
MIA
Maternity Immunisation Allowance
Social Policy Research Centre 2017
iii
Executive summary
The Australian Government Department of Social Services (DSS) commissioned the
Social Policy Research Centre (SPRC) at UNSW Sydney to undertake a Post
Implementation Review (PIR) of the
No Jab, No Pay 2015 Budget measure (the Measure).
The intended outcomes of this review were:
•
to determine whether the Measure was implemented effectively by measuring
successes and challenges that have been encountered in the first 6–12 months of
the Measure's implementation
•
to provide a framework for the subsequent impact evaluation.
The PIR was undertaken to assess implementation successes and challenges and also to
inform the development of the impact evaluation framework. The PIR was guided by
several key questions:
Policy design
Has implementation been consistent with the Measure's policy design?
If there have been any deviations from the original design, have these been
positive or negative in nature?
Issues and risks
What successes and challenges (including design, system, data, communications,
and uptake of immunisation by the target populations) were encountered in
implementing the Measure?
Governance
Did governance and decision-making mechanisms help or hinder the successful
implementation of the Measure?
Service delivery
Has the service delivery model resulted in impacted recipients having positive or
negative encounters?
Communications Did the communication strategy and Departmental communication plans
successfully support the implementation of the Measure?
Did the Communication Working Group effectively manage communication issues
as they arose?
Management
How has the policy and system design impacted upon the data available to date
information
regarding rates of immunisation and eligibility for both family assistance (Family
Tax Benefit Part A supplement) and child care payments?
The methodology for the PIR included:
• a document review of publicly available and internal documents from the four
departments involved in implementing the Measure: DSS, Department of Human
Services (DHS), Department of Health (Health) and Department of Education and
Training (DET)
Social Policy Research Centre 2017
4
• a data scoping exercise
• qualitative stakeholder consultation with 17 government and external stakeholders
• a workshop with departmental staff involved in implementing the Measure.
The data gathered through these sources were analysed and synthesised in order to
answer the research questions guiding the PIR.
Policy design
The rationale of successive governments in placing mutual obligations on recipients of
social security and family assistance payments is based on the concept of encouraging
behaviours beneficial to individuals and the broader community. Conditionality is a key
priority of the government, and this was reflected in the design of the No Jab, No Pay
policy in setting out specific immunisation requirements that a child must meet to be
eligible to receive a benefit or payment. The policy’s intent sought to reinforce the
importance of immunisation as a measure to ‘protect public health’ and highlight that the
choice made by families to not immunise children should not be supported by taxpayers in
the form of government benefits.
The policy was designed to extend existing immunisation eligibility requirements for child
care and family payments through three key mechanisms:
• removal of vaccination objection as a valid exemption category
• requirement for individuals up to 20 years of age to be fully vaccinated to receive
family payments
• removal of the 63-day initial grace period for new child care claimants to either get
up to date with immunisations or commence a catch-up schedule.
The review found that implementation was consistent with the Measure's policy design.
Activation of the three mechanisms was supported by the detailed implementation plans
from DSS and DHS, with the latter outlining the expansion of the Australian Childhood
Immunisation Register (ACIR) to the Australian Immunisation Register (AIR).
Implementation was also supported by the complementary measures introduced by
Health.
Most stakeholders felt that the implementation of the Measure had been consistent with
the policy’s design. While the policy had undergone some minor changes since it was
originally announced, these were generally carried out well before the Measure was
launched and did not constitute significant deviations from the policy design.
Two key implementation challenges concerned the need to:
• extend the payments beyond the initial grace period for existing recipients to
prevent parents from losing access to child care payments when their child’s
immunisations were up to date but the ACIR records did not reflect this (due to
delays in states/territories updating the ACIR)
Social Policy Research Centre 2017
5
• amend the continuous/rolling catch-up anomaly which could have enabled parents
to delay vaccination indefinitely and continue to receive family payments.
Both of these were addressed promptly and appear to have prevented any negative
impacts for recipients, and supported the policy’s initial design.
A further challenge identified by stakeholders concerned the eight-month timeframe
between the policy announcement and its implementation. Key implementation challenges
included the changes to the ACIR, the uncertainty around when the legislation would pass
and limited timeframes for engaging and communicating with stakeholders. The tight
timeframe appears to have presented difficulties for health service providers at state and
territory level who were responsible for immunising children.
Issues and risks
A number of procedures were put in place to identify issues and risks that could negatively
affect implementation of the Measure. These included:
•
an issues register and risk log maintained by DSS
•
an issues register maintained by DHS
•
the establishment of an Interdepartmental Committee (IDC) with Senior Executive
staff and an Executive Level working group were also key to identifying, discussing
and strategising to mitigate issues and risks.
Identified challenges with respect to policy design included: calls in social media for a High
Court challenge to the legality of the Measure; feasibility of using the Secretary’s
Exemption to address challenging clinical circumstances; fraudulent medical exemption
forms; and eligibility monitoring. Identified system challenges included:
• Australian Government and state/territory interactions in the case of delays in
states/territories uploading immunisation data to the ACIR
• vaccine availability.
Identified data challenges included concerns about the quality of the data in the ACIR,
delays in uploading data, and the ability to monitor vaccination objection. An additional
system challenge was the increased workload for state/territory services, including local
councils, public health units and vaccination providers, who reported that they were
overwhelmed by the increased workload associated with the commencement of the
Measure.
s47E(d)
Social Policy Research Centre 2017
6
Governance
The governance structure established for the Measure included a high level (Senior
Executive) Interdepartmental Committee (IDC) and an Executive Level Working Group that
both met regularly to handle practical implementation issues. These were in addition to the
‘business as usual’ governance arrangements in each agency. There was also a separate
Communications sub-committee, as well as some department-specific steering
committees. These governance structures were effective in identifying, and strategising to
mitigate issues and risks.
Service delivery
The stakeholder consultation provided some insight into whether recipients had positive or
negative encounters with service provision. Australian Government and external
stakeholders held divergent views about this. Most government stakeholders felt that
recipients had a positive experience with the new requirements, which they attributed to
the public’s acceptance of the overall aims of the Measure. Government stakeholders
nominated two areas in which recipients’ experiences were negative. These centred on
confusion for recipients around the process of updating their children’s vaccination details
(and delays in having ACIR records updated), and vaccination objectors’ opposition to the
Measure. The external stakeholders characterised recipients’ experiences with
implementation of the Measure more negatively. They felt that recipients’ experiences
were dependent on their child’s vaccination status, highlighting the difficulties faced by
many parents whose children were immunised overseas in fulfilling their obligations, as
well as the perceived inadequate communication around the Measure from government.
External stakeholders felt that a lack of knowledge and confusion around the impact of the
Measure caused anxiety for many parents.
Communications
The Measure’s communication activities were the joint responsibility of DSS, Health, DHS,
and DET, with the DSS’ strategy outlining the agreed overarching communication
approach. Complementary communication strategies were developed by DHS and Health.
Communication activities were undertaken by DSS to inform parents, service providers
and other stakeholders of the changes. Health developed a communication plan for
vaccination providers, including general practitioners. DHS also developed a
communication implementation plan and undertook a range of communication activities
including: general information letters for recipients, letters for CCB recipients, letters for
FTB recipients, and additional letters for parents whose child/ren’s immunisation status
was either not up to date, unknown (because child was not linked) or was mismatched with
information on file. DET was responsible for communicating with child care services via the
Child Care Management System (CCMS) Helpdesk.
Most government stakeholders agreed that the Measure’s communications strategy,
including letters to recipients and health providers, as well as general media, was effective
in supporting implementation. Nevertheless, many were aware of issues that hampered
Social Policy Research Centre 2017
7
communications, including: the tight timeframe for implementation resulting in delays in
getting information to recipients and health professionals, the complexity of the message
and confusion due to different requirements for different payments. Positive outcomes of
the communications strategy included consistency in delivering the same message across
departments and utilising as many channels as possible to communicate the changes
resulting in high levels of awareness. External stakeholders were generally less positive
about communications surrounding the Measure. Most reported that they had not received
adequate information about the Measure, or that there were gaps in the information
provided which hindered their ability to explain the changes to recipients.
Management information
The document review highlighted concerns about the completeness of the data in the
ACIR, the capacity to monitor vaccination objectors in the future, concerns about data
linkages and the management information that was produced to monitor implementation
and impact.
Stakeholders noted that implementing the Measure necessitated a significant amount of
additional information being entered into the ACIR, as children aged 10 up to 20 years now
needed full vaccination histories recorded. Linkages between the Centrelink payment
database and the ACIR also needed to be updated. Several government and external
stakeholders commented that the ACIR had improved, but that some short-term issues
were experienced, including delays uploading data, data cleansing and parental angst.
Other government stakeholders referred to the additional work to establish linkages
between DHS and the ACIR. It was acknowledged that the process was not without its
challenges but that linkages were ultimately successfully established.
Regular reports from Centrelink (DHS) data were provided to DSS, DET and Health to
determine whether the Measure had resulted in any changes to the number of families
receiving payments. Minutes from meetings of the IDC and the Working Group provide
some information about the impact of the Measure on child care payments and on FTB
Part A supplement payments.
The impact evaluation should examine the quality of the data on immunisation rates in the
ACIR. While the ACIR contains historical information on registered vaccine objections, the
capacity to monitor ongoing levels of vaccine objection in the community has reduced.
Options to continue to monitor vaccination objection, as part of a broader inquiry into
community understanding and confidence in vaccines, should be examined as suggested
by submissions to the Senate Inquiry.
PIR summary conclusions
Overall, the implementation of the Measure went relatively smoothly from a policy
perspective. Governance arrangements, risk mitigation strategies and communication
strategies were put into place, and the Measure was implemented in a flexible manner that
allowed for challenges to be addressed as they arose. Government departments worked
well together and the communication between departments was effective in addressing
Social Policy Research Centre 2017
8
overlaps and gaps. There were additional benefits to the implementation of the Measure,
in particular improvements in the completeness of data in the ACIR.
Despite the effective implementation by the Australian Government there were
considerable difficulties for state and territory officials as well as vaccination providers.
Some of these difficulties resulted from the parameters of the Measure itself. These
included:
• the short timeframes for implementation
• the perceived lack of additional resources provided for states and vaccine
providers, other than the $6 incentive for catching-up overdue children
• the incompleteness of the AIR and backlogs in getting data uploaded onto the
register.
Other challenges may have been better addressed in the implementation, in particular, that
only three states sought additional support for implementing the Measure via primary
health networks, and the perceived inadequacies in support available for state and territory
vaccine providers, despite regular meetings with the Australian Government departments
during implementation.
Overall, the majority of the challenges can be accounted for as ‘teething problems’, which
are to some extent inevitable in the implementation of any complex measure, particularly
when it is required in a short time frame. It is anticipated that most of these challenges will
be resolved and will not affect implementation in the long-term. Perhaps the only long-term
unintended consequence of the Measure has been the loss of ability to track vaccine
objectors and henceforth the Government will need to rely on proxy measures to assess
the extent of vaccination objection in the community.
Although the early implementation has been mostly successfully accomplished, it is not yet
possible to assess whether the Measure itself has been successful. There are early
indications that vaccination rates have improved, but it is not possible at this stage to
attribute changes to the Measure or any particular component of it. An impact evaluation
would need to be undertaken to assess the degree to which the Measure has not only
improved administrative processes, but has led to actual changes in population behaviour,
and whether these have been sustained over time.
The most contentious aspect of the Measure concerns the underlying theory of change,
the long-term effectiveness of a sanctions-based approach as opposed to an incentive-
based approach to public health, and the unintended consequences for children who are
not up to date with vaccinations because of issues other than vaccination objection. These
questions will be tested in any impact evaluation.
Impact Evaluation
Drawing on insights gained through the PIR, options and strategies for conducting the
impact evaluation of the Measure were also developed.
Social Policy Research Centre 2017
9
Two key challenges for any impact evaluation relate to isolating the impact of the Measure
on immunisation rates and trying to establish a baseline measure for determining impact.
As noted in the theory of change model, a range of additional contextual factors may have
had an impact on the immunisation rates. These include state-based policies,
complementary measures introduced by Health and media coverage of vaccination. As
such, isolating the impact of the Measure on immunisation rates will be a challenge. It may
be possible to examine the impact of outside factors through qualitative research, which
should complement the administrative data analysis.
The key questions to be addressed in any impact evaluation would be:
• Did the Measure achieve its intended goal of increasing immunisation rates and
achieving herd immunity in the Australian population?
• To what extent can changes in immunisation rates be attributed to the Measure?
• Were there any unintended impacts (positive or negative) of the Measure?
• Is the Measure cost-effective? (cost benefit analysis)
• Have there been any ongoing implementation challenges following the post-
implementation phase?
We recommend that any impact evaluation adopt a ‘before and after’ mixed method
design, as it will not be possible to utilise a counterfactual or comparison group to assess
impact.
The economic evaluation could draw upon the findings of any impact evaluation and will
model the economic costs and benefits of vaccinating additional children after the onset of
the Measure. Where possible, this analysis will include a geographical breakdown, as the
benefits of vaccinating a child living in an area with low vaccination rates will be greater
than a child living in an area with already high rates of vaccination. Similarly, if possible,
the modelling will include vulnerable groups such as Aboriginal and Torres Strait Islander
and CALD children who are at higher risk of vaccine-preventable disease. A broad
estimate of the costs of the evaluation would be around $400,000.
Social Policy Research Centre 2017
10
1 Introduction
The Australian Government Department of Social Services commissioned the Social
Policy Research Centre (SPRC) at UNSW Sydney to undertake a Post Implementation
Review (PIR) of the No Jab, No Pay
2015 Budget measure. The intended outcomes of this
review were:
• to determine whether the Measure was implemented effectively by measuring
successes and challenges that have been encountered in the first 6–12 months of
the Measure's implementation
• to provide a framework for the subsequent impact evaluation.
The report is divided into two main parts: the first presents the findings of the PIR, and the
second outlines a framework for an impact evaluation of the No Jab, No Pay
2015 Budget
measure.
The findings of the PIR are further subdivided. We begin by presenting a select review of
the literature on the impact of similar measures. In the following section, we present the
methodology for the PIR, the research questions guiding the PIR and present the findings
from the document review, the stakeholder consultation and data scoping exercise.
In part two, we present an impact evaluation framework.
Social Policy Research Centre 2017
11
link to page 94 link to page 96 link to page 94 link to page 94 link to page 96 link to page 96 link to page 96 link to page 95 link to page 96 link to page 96
2 Literature review
This section presents a select review of the literature with a view to providing some
background to immunisation rates in Australia, interventions designed to increase
immunisation rates and the introduction of the Measure. The review is by no means
exhaustive; rather it aims to provide some context for the PIR.
Immunisation is considered to be a highly effective and cost-effective health intervention
and increasing immunisation rates is a key public health goal at both the national and
global level
(Australian Government, 2014; World Health Organization, 2013). Routine
immunisations for infants began in Australia in the 1950s when immunisation was the
responsibility of individual states and territories. Over time, however, disparities in
immunisation rates between states and territories became evident, with differences
attributed to differential funding of, and access to, vaccines. A national survey in the 1980s
indicated that only 53 per cent of children were adequately immunised. Concern about low
rates of immunisation led to the development of the first National Immunisation Strategy in
1993 and the establishment of the Australian Childhood Immunisation Register
(ACIR) in
1996
(Australian Government, 2014).
In 1997, the
Immunise Australia: Seven Point Plan was launched to increase childhood
immunisation rates. The aim of this program was to increase vaccination rates among the
general population. Strategies to increase immunisation rates introduced under the
Seven
Point Plan included financial incentives for parents and general practitioners, improved
methods for monitoring vaccination coverage, education, research and school entry
requirements
(Australian Government, 2014; Pearce, Marshall, Bedford, & Lynch, 2015;
Ward, Hull, & Leask, 2013).
Under the
Immunise Australia: Seven Point Plan, immunisation status was linked to the
Maternity Immunisation Allowance (MIA) and child care payments (‘Child Care Assistance
Rebate and/or the Child Care Cash Rebate’). Depending on factors such as income, size
of family and type of child care, rebates ranged from $20–$122 for every child per week.
The MIA was a one off payment of $200 for every child that was fully immunised at 19
months of age
(Ward et al., 2013). In order to remain eligible for these payments, parents
were required to provide evidence that their child was fully immunised according to the
immunisation schedule included in the National Immunisation Program (NIP). Parents who
disagreed with vaccination or had philosophical reasons for not having their children
vaccinated could register as ‘conscientious objectors’ in order to continue receiving these
payments
(Lawrence, MacIntyre, Hull, & McIntyre 2004).
The MIA was modified in 2009 and ceased in 2012, and immunisation status was linked to
the existing means-tested Family Tax Benefit (FTB) Part A supplement at ages 1, 2 and 5
years. Parents were exempt from the immunisation requirements if they registered their
‘conscientious objection’1 with DHS
(Ward et al., 2013). Ward, Chow, King, and Leask
1 Based on the data available on the ACIR website, it appears that the recording of conscientious objection
data commenced in 1999.
Social Policy Research Centre 2017
12
link to page 96 link to page 95 link to page 95 link to page 96 link to page 96 link to page 96 link to page 95 link to page 95 link to page 95 link to page 96 link to page 94 link to page 94 link to page 96 link to page 94
(2012) argue that ‘[l]egislated parental incentives for childhood immunisation have been
broadly accepted among Australian parents and have had a positive impact on uptake and
timeliness’.
Data on children’s immunisation status was held in the Australian Childhood Immunisation
Register (ACIR) (now the Australian Immunisation Register (AIR)). The ACIR was
established in 1996 and included the immunisation data for children registered with
Medicare—roughly 99 per cent of children in Australia
(Hull et al., 2013, p. 149). The
register relied on general practitioners and other vaccination providers reporting
vaccination information to the ACIR after administering vaccines. Children vaccinated
overseas were required to provide proof of vaccinations to Australian vaccination
providers, who entered the information in the ACIR. Proof of vaccination was required for
data to be submitted to ACIR
(Gibbs, Hoskins, & Effler, 2015).
Under the
Seven Point Plan, a General Practice Immunisation Incentive scheme (GPII)
was introduced. The aim of the scheme was to encourage general practitioners to notify
the ACIR of changes of immunisation status of children under 7 who came to their
practice. Under the scheme, general practitioners received a $6 payment for each
notification that a child has been fully immunised according to the schedule
(Ward et al.,
2013). GPII also paid performance funding to general practitioners able to demonstrate
immunisation coverage above 90 per cent for their practice. With respect to child care
attendance, children for whom conscientious objection to vaccination had been registered
could still attend, but could be temporarily excluded in the case of an outbreak of a
vaccine-preventable disease
(Salmon et al., 2006).
The implementation of the
Seven Point Plan led to dramatic increases in vaccination rates
among children. Between 1996 and 2000, vaccination coverage among children aged 12
months increased rapidly to over 90 per cent of infants aged 12–15 months. However,
uptake has since remained relatively stable at around 91 to 92 per cent
(Hull et al., 2013,
p. 164), which is below the OECD average and falls below the levels required for herd
immunity for some diseases
(Harvey, Reissland, & Mason, 2015; Pearce et al., 2015). The
Australian Government Chief Medical Officer and the state Chief Health Officer agreed to
an aspirational target of 95 per cent immunisation coverage rates, consistent with the
World Health Organization’s Western Pacific Region target. This is the level required to
achieve ‘herd immunity’
(Department of Health, 2016). Herd immunity refers to the
required percentage of the population that needs to be vaccinated to prevent the outbreak
of vaccine-preventable diseases
(Danchin & Nolan, 2014). Although the proportion differs
for different diseases, the WHO Western Pacific Region’s standard, based on measles, is
95 per cent of the population
(Wigham et al., 2014, p. 1118). The figure is a whole of
population target, but ideally 95 per cent of the population should be immunised in every
geographic community.
2.1 Immunisation rates
The National Immunisation Program Schedule provides a list of vaccinations that all
Australian children are expected to receive and the age at which they are expected to be
administered
(Australian Government, 2016c). It also identifies the vaccinations to be
Social Policy Research Centre 2017
13
link to page 94 link to page 94 link to page 94 link to page 94 link to page 94 link to page 95 link to page 96 link to page 95 link to page 96 link to page 96 link to page 96 link to page 94
provided through school vaccination programs, additional vaccinations that Aboriginal and
Torres Strait Islander children should receive and additional vaccinations for other ‘at-risk’
groups.
Coverage data for children aged 24 months in 2014 from the ACIR indicate that 91.23 per
cent were up to date with their immunisations. Of the remaining children, 7 per cent were
not up to date with their immunisations and did not have a recorded conscientious
objection, and just 1.77 per cent had a recorded conscientious objection
(Australian
Government, 2016a). These figures suggest that most children’s incomplete vaccination
status are likely to be attributable to causes other than vaccine refusal
(Beard, Hull, Leask,
Dey, & McIntyre, 2016). The picture is complicated by a number of factors, including that
some parents who registered as conscientious objectors nevertheless went on to
vaccinate their children, and also that some children were not registered on the ACIR at
all. Thus the exact proportion of conscientious objectors is difficult to determine.
Nevertheless, it is a very small proportion of the total population.
2.2 Factors contributing to incomplete childhood immunisation
With immunisation rates below the national aspirational immunisation coverage target,
researchers have sought to explore the characteristics of partially and non-immunised
children. The literature identifies two key groups of parents whose children are not
immunised at all or are incompletely immunised. The first group consists of parents who
face barriers to accessing immunisations ‘which may relate to social disadvantage and
logistical barriers’
(Beard et al., 2016; Leask et al., 2012; Pearce et al., 2015). The second
group consists of parents who hold concerns about the safety of vaccines: so-called
‘vaccine hesitators’
(Leask et al., 2012).
2.2.1 Socio-economic disadvantage and logistical barriers
In their analysis of data from the Longitudinal Study of Australian Children (LSAC),
Pearce
et al. (2015) found that the majority of incompletely immunised infants (in 2004) did not
have a mother who disagreed with immunisation. Barriers to complete immunisation
identified in the study were: having a larger family (three or more children), moving house
since the birth of the child, less than weekly contact with friends and family, and the use of
formal group childcare. The parents of children who were incompletely immunised had
lower education and income levels.
Ward et al. (2012) also note that certain groups,
including Aboriginal and Torres Strait Islander people and those living in socio-economic
disadvantage, were more likely to be incompletely immunised.
Beard et al. (2016) found that partially vaccinated children without a registered
conscientious objection were more likely to be living in areas in the lowest decile of socio-
economic status, ‘suggesting delayed vaccination caused by problems related to
disadvantage, logistic difficulties, access to health services, and missed opportunities in
primary, secondary and tertiary health care’ (p. 275). They also found that children born
overseas were significantly more likely to have neither vaccinations nor an objection
recorded, but acknowledged that they may very well be vaccinated.
Social Policy Research Centre 2017
14
link to page 95 link to page 94 link to page 95 link to page 95 link to page 94 link to page 94
Gibbs et al. (2015) found that the most commonly reported reason why a significant
minority of children in Western Australia had no vaccination history recorded in the ACIR
was because their families had moved from overseas and their vaccination history had not
been recorded in the ACIR. The second most common reason was that the parents were
unregistered conscientious objectors.
2.2.2 Vaccine hesitancy
Forbes at al. (2015) define vaccine hesitancy as having varying degrees of concerns about
immunisation. They estimate that between 30 and 70 per cent of parents in developed
countries could be categorised as vaccine-hesitant. Reasons for vaccine hesitancy include
religious obligations, safety concerns for children, distrust of government services and
health systems, misinformation or lack of knowledge, and the perceived threat of autism
following vaccinations
(Danchin & Nolan, 2014; Dubé et al., 2016). Despite the empirical
literature reinforcing the benefits and safety of vaccinations, vaccine hesitancy continues to
rise
(Dubé et al., 2016).
Vaccine hesitancy can lead some parents to delay vaccination, to select only the vaccines
they consider safe or to outright refuse to vaccinate. Prior to 1 January 2016, parents who
refused to vaccinate their child could continue to access child care payments if they
registered a ‘conscientious objection’ with DHS (via a recognised immunisation provider).
Parents who chose not to vaccinate and who were ineligible for payments could register an
objection if they wished.
In their analysis of trends and patterns in vaccine objection between 2002 and 2013 as
recorded in the ACIR,
Beard et al. (2016) found that the proportion of children with a
registered objection increased from 1.1 per cent to 2.0 per cent. They found that children
with a registered objection were clustered in regional areas, which they note can pose a
risk of local disease outbreak. They also found that children with a registered objection
were more likely to be living in areas in the highest socio-economic decile than in the
lowest. This implies that financial sanctions, such as the withdrawal of FTB Part A
supplement, are less likely to impact on those with a registered objection than on vaccine
hesitators and those whose children have not been fully vaccinated because of logistical
barriers. However, Child Care Rebate is not subject to a means test, and as such is likely
to have an impact across all socio-economic deciles.
2.3 Increasing immunisation uptake
Improving vaccination uptake is a key policy goal both nationally and globally, with a range
of different approaches adopted with this goal in mind. Measures include: financial
incentives, financial penalties, reminder systems, and effective communication/education
strategies. Often a combination of different approaches is adopted. Much Australian and
international research has sought to evaluate the impact of these approaches on
increasing immunisation rates, with many considering the cost-effectiveness of the
approaches. Prior to considering some of this research, it is important to note that many
authors acknowledge the poor evidence-base for determining the most effective
strategies/interventions for increasing vaccine uptake, and the need for the rigorous
evaluation of any intervention and its impact on vaccine hesitancy/refusal
(Dube, Gagnon,
Social Policy Research Centre 2017
15
link to page 94 link to page 95 link to page 95 link to page 96 link to page 95 link to page 96 link to page 95 link to page 96 link to page 96 link to page 95 link to page 95 link to page 95 link to page 95 link to page 95 link to page 95 link to page 95 link to page 94
MacDonald, & The SAGE Working group on Vaccine Hesitancy, 2015; Leask, Willaby, &
Kaufman, 2014; Williams, 2014).
2.3.1 Financial incentives
Since the
Seven Point Plan, policy makers in Australia have used financial incentives to
increase vaccination rates
(Lawrence et al., 2004; Ward et al., 2013). Although vaccination
rates increased significantly following the introduction of the Plan
(Hull et al., 2013), other
reforms, including educational campaigns, financial incentives for general practitioners and
school/childcare entry requirements, were introduced at the same time. This makes it
difficult to separate the impact of financial incentives on the increase
(Ward et al., 2013).
Neverthel
ess, Ward et al. (2013) argue that they ‘are likely to have made a significant
contribution to increasing childhood immunisation coverage to over 90%’ (2013: 592).
However, overall, there is limited empirical evidence documenting the effectiveness of
financial incentives on vaccination behaviour
(Lawrence et al., 2004; Mantzari, Vogt,
Marteau, & Kazak, 2015).
A perceived risk of incentivising parents to immunise their children by offering a financial
reward is that they may feel more compelled to vaccinate for the financial rather than
health benefits. For this reason, financial rewards are often combined with educational
programs and other interventions aimed at increasing vaccination uptake
(Mantzari et al.,
2015).
2.3.2 Financial penalties
Several studies have examined the effectiveness of financial sanctions on immunisation
rates. In many cases, however, financial sanctions are introduced alongside other
changes, making it difficult to isolate their effectiveness alone.
An Australian study by Lawrence et al. (2004) sought to determine if the risk of financial
sanction influenced parents’ decision to vaccinate. Overall the study found an association
between knowledge of welfare payments and age-appropriate vaccinations. However, it
also highlighted that encouragement from health care professionals was important in the
decision-making process. Among parents whose children were fully immunised, only 4.4
per cent reported that the MIA was the most important influence on their decision to
vaccinate, while for 0.7 per cent of parents, it was the Child Care Benefit (CCB)
(Lawrence
et al., 2004). Roughly two thirds of the parents in the study who received the MIA indicated
that they were vaccine-hesitant. This may indicate that linking welfare payments with
vaccinations may be influential in increasing vaccination uptake amongst this group.
Given the increase in the number of school-age children receiving vaccine exemptions for
non-medical reasons in the United States
, Constable, Blank, and Caplan (2014) argue that
measures that impose a financial cost on vaccine objection ought to be considered
alongside more effective vaccination education in order to increase vaccination rates. They
acknowledge that imposing a financial penalty (e.g. financial incentives in the form of
taxation, health insurance costs, and or private school funding) ‘falls somewhere on the
spectrum between persuasion and coercion’ but argue that the public health benefits
outweigh this imposition on autonomous decision-making.
Social Policy Research Centre 2017
16
link to page 94 link to page 94 link to page 95 link to page 95 link to page 96 link to page 94 link to page 95 link to page 95 link to page 95
The use of financial sanctions to encourage vaccination uptake has raised ethical
concerns internationally
(Adams et al., 2016). Concerns relate to the perceived removal of
civil liberties, penalising children for their parents’ decisions, and increasing families’
financial hardship. While financial sanctions can lead to increases in vaccination uptake,
they may also disengage vaccine hesitant parents and health professionals from the
educational process. On the other hand, it could be argued that the public health benefits
of vaccinations may outweigh individuals’ right to decide whether or not they vaccinate
(Adams et al., 2016). The challenge is to find the right balance between the right to
autonomy and the right for safety from vaccine-preventable diseases.
2.3.3 Reminder systems and follow-up
Harvey et al.’s
(2015) systematic review and meta-analysis found that receiving both
postal and telephone reminders was the most effective reminder-based intervention for
increasing vaccination uptake, and that educational interventions were more effective in
low- and middle-income countries. In their systematic review,
Jacob et al. (2016) found
that reminder systems, for clients or immunisation providers, were among the lowest cost
strategies to implement and the most cost-effective in terms increasing immunisation rates.
They found that strategies involving home visits and combination strategies in community
settings were expensive and less cost-effective.
Ward et al.’s (2012) systematic review identified a number of strategies to improve
vaccination uptake that were relevant to the Australian context. Of the strategies reviewed,
catch-up plans showed the greatest impact on immunisation uptake but recall/reminders
for patients and vaccination providers were the most commonly evaluated strategies and
had the strongest evidence.
In the Australian context,
Pearce et al. (2015) argue that greater effort should focussed on
overcoming barriers to immunisation through sending reminders and rescheduling
cancelled appointments or interventions that offer immunisation in alternative settings for
those families that face challenges accessing services.
Given that a high proportion of incompletely immunised children in their analysis had
moved from overseas,
Beard et al. (2016) recommend that primary care clinicians should
focus on both partially vaccinated children and overseas born children. For the latter their
overseas vaccination history should be accurately confirmed by a vaccination provider and
recorded in the ACIR. This is echoed by
Gibbs et al. (2015) who recommend a number of
strategies for addressing the immunisation status and records of families moving from
overseas.
2.3.4 Effective clinician communication
Researchers have emphasised the importance of effective clinician communication for
increasing vaccination uptake.
Forbes, McMinn, Crawford, Leask, and Danchin (2015) differentiate between five groups of parents based on their stance towards immunisation.
These are: unquestioning acceptors, cautious acceptors, hesitant vaccinators, late or
selective vaccinators and refusers. Elsewher
e, Leask et al. (2012) develop a framework to
assist clinicians in communicating effectively with these different groups of parents to
Social Policy Research Centre 2017
17
link to page 95 link to page 95 link to page 95 link to page 94 link to page 95 link to page 96 link to page 96
enable them to make informed decisions about vaccination. In emphasising the centrality
of effective clinician-parent dialogue, regardless of the parent's stance towards
immunisation, Leask et al. advocate for ‘an approach to communication that encourages
questions and employs a guiding rather than directing style’.
In advocating for the need for ‘new approaches to vaccine consultation’
, Leask and
Kinnersley (2016) argue that physicians need to have the opportunity to engage with
vaccine-hesitant parents in order to address any concerns they might have. They
acknowledge that physicians are generally unable to devote adequate time to undertake
training in communication interventions, and suggest that decision aids that ‘are designed
to help people understand their options and potential outcomes, to consider the possible
benefits and harms of their choices, and to increase consumer participation in decision-
making’ might prove useful in the context of vaccine hesitancy. They argue that it is critical
that funding is directed towards developing ‘conceptually clear, evidence informed, and
practically implementable approaches to parental vaccine hesitancy’.
Elsewher
e, Leask (2015) argues against an adversarial approach to increasing vaccination
rates, because it draws attention to vaccination objectors and their arguments and has the
potential to alienate vaccine-hesitant parents. Instead, she argues that advocacy and
policies should address the factors that influence the low uptake of vaccines.
Leask et al (2014)'s article on vaccine hesitancy outlines a number of strategies that are
required in order to address vaccine hesitancy. These include: the identification and testing
by governments and research agencies of interventions designed to increase uptake of
vaccines among vaccine-hesitant parents; monitoring vaccine acceptance; community-
level responses to engage communities in dialogue (as vaccination rejection or hesitancy
is often a community-based phenomenon); provider-level solutions as interaction between
parents and providers can influence uptake, however the evidence-base is limited; and
provider education – vaccination providers ought to have a good understanding of
vaccines and vaccine hesitancy. Addressing vaccine hesitancy requires ‘political will,
professional commitment, and research investment in order to develop and evaluate new
and innovative solutions’ (p. 2601).
The extant evidence suggests that the most effective interventions for increasing
vaccination rates involve multi-component strategies which generally include educational
programmes and interventions which aim to address logistical barriers to immunisation
(Dube et al., 2015; Jarret, Wilson, O’Leary, Eckersberger, & Larson, 2015; Pearce et al.,
2015). Because most interventions include several components, it is often difficult to
determine which component or combination of components leads to an increased
vaccination uptake. As there are multiple population groups who do not fully vaccinate their
children, with different drivers for each group, it is likely that no single measure – or type of
measure – will address the needs of all these groups, and that multi-component strategies
will need to specifically target conscientious objectors, vaccine hesitators and those who
face logistical barriers to having their children vaccinated.
Social Policy Research Centre 2017
18
link to page 95 link to page 96 link to page 94
2.4 The No Jab No Pay budget measure
On 12 April 2015, the Measure was announced by the Hon Scott Morrison MP, the then
Minister for Social Services and the then Prime Minister the Hon Tony Abbott MP. The
Measure was a pre-budget Government announcement and was included in the 2015–16
Australian Government Budget. From 1 January 2016, the Measure was implemented by
the Australian Government. There is as yet no available research evidence about the
impact of the Measure on immunisation rates; however, some commentary on the
Measure appeared shortly after its announcement in 2015.
In an opinion piece in the Australian Medical Association's (AMA) publication
Australian
Medicine, Macartney (2015) of the National Centre for Immunisation Research &
Surveillance argues that there are better ways to improve vaccination rates than imposing
financial penalties on parents. She asserted that the Measure is 'unnecessarily punitive
and could have negative repercussions' and that there are alternative means of increasing
the immunisation rate. These include: reminding and supporting parents to immunise;
improving access, awareness and the affordability of vaccination; enabling vaccine-
hesitant parents to engage with qualified health professionals; and grassroots campaigning
for immunisation that promotes immunisation as part of a healthy lifestyle.
In the
Australian Medicine Budget edition (14 May 2015),
Rollins (2015) highlighted the
AMA’s concern about the projected savings to government of over $500 million by 2018–
19 from the Measure, because families will be ineligible for child care payments and family
tax benefits. Rollins quotes the President of the AMA as stating that the aim should be to
invest the money saved on increasing vaccination rates.
While some external stakeholders focussed on the perceived savings, the Government
made it clear that the purpose of the Measure was to improve immunisation rates, not
budgetary savings
(Abbott, 2015). These concerns, and the lack of empirical evidence in
Australia and internationally about the effectiveness of different strategies to increase
vaccination rates, make it imperative that the Measure should be comprehensively and
independently evaluated to examine its impact on different population groups in the short,
medium and longer term.
Social Policy Research Centre 2017
19
link to page 22
3 Methodology
The No Jab, No Pay Post Implementation Review was guided by several key questions
listed below. As shown in
Table 1 the methodology drew upon different methods of data
collection to address each question.
Table 1 Research areas, questions and data sources
Research questions
Data sources
Policy design
1. Has implementation been consistent with the Measure's policy design?
Document review
2. If there have been any deviations from the original design, have these been
Stakeholder
positive or negative in nature?
consultations
Data scoping
Issues and risks
1.
Stakeholder
What successes and challenges (including design, system, data,
consultations
communications, and uptake of immunisation by the target populations) were
encountered in implementing the Measure?
Document review
Governance
1. Did governance and decision-making mechanisms help or hinder the successful Stakeholder
implementation of the Measure?
consultations
Document review
Service delivery
Stakeholder
1. Has the service delivery model resulted in impacted recipients having positive
consultations
or negative encounters?
Communications
Stakeholder
1. Did the communication strategy and Departmental communication plans
consultations
successfully support the implementation of the Measure?
2. Did the Communication Working Group effectively manage communication
Document review
issues as they arose?
Management information
Data scoping
1. How has the policy and system design impacted upon the data available to date
regarding rates of immunisation and eligibility for both family assistance (Family
Stakeholder consultation
Tax Benefit Part A supplement) and child care payments?
Social Policy Research Centre 2017
20
3.1 Document review
The document review involved a review of publicly available and internal government
documents. The Department of Social Services (DSS) provided the research team with
documents and web links under the following headings:
• Senate Community Affairs Legislation Committee Inquiry
• Reports and Project Plans
• Fact sheets and schedules
• Policy resources
• Legislation
• Data sets
• Communications
• Letters to recipients
• No Jab, No Pay Interdepartmental Committee and Working Group papers.
These documents were imported into the qualitative software NVivo where they were
coded and reviewed.
3.2 Data scoping
The review of the datasets involved a data scoping exercise that provided the research
team with an understanding of the quality of data available and the degree to which it may
be useful for inclusion in the subsequent impact evaluation. The review did not involve any
analysis of the available data. The data scoping encompassed a review of four data
sources, as advised by the DSS: the ACIR/AIR, Child Care Management system, Day One
implementation reports and data from the Enterprise Data warehouse in DHS. Discussions
about the data items, data quality, data linkage processes and departmental processes for
data access for external researchers were conducted with key contacts from DSS, DHS,
DET and ACIR/AIR. Data dictionaries were requested in all cases and provided by DHS.
3.3 Qualitative stakeholder consultation
A component of the PIR involved consultation with key staff in the four government
departments (DSS, Health, DHS, DET) involved in the implementation of the Measure and
with stakeholders from organisations external to the Australian Government. Fifteen staff
members from the four government departments and eight external stakeholders were
invited to participate in semi-structured interviews. Ethics approval for the PIR was given
by the UNSW Australia Human Research Ethics Committee (HREC No. HC16563) and
participation in the research was voluntary.
Nine government stakeholders were interviewed from DSS, Health, DHS, DET. These
stakeholders were from a range of areas within these departments, including payment
policy and operations, immunisation policy and programs, database management, and
communications. In addition, nearly all of these stakeholders were involved with both the
Working Group and the Interdepartmental Committee. Most had also been involved in the
design and development of the policy prior to its implementation.
Social Policy Research Centre 2017
21
link to page 96
In addition to the government stakeholder cohort, eight external stakeholders were
interviewed. These external stakeholders were from organisations external to the
Australian Government, with four representing state-based health service providers, two
representing a not-for-profit early learning provider, one representing a peak body, and
one academic. As such, their perspectives differed from those of the government
stakeholders as they had less of an ‘internal’ view of the implementation and more of an
‘on the ground’ view, allowing them to comment on the effects of the Measure on
immunisation providers and recipients. The interviews were conducted over the phone and
recorded with participants’ consent.
It is important to emphasise that the views gathered through the stakeholder consultation
are not necessarily representative of all individuals involved in the implementation of the
Measure. Rather, qualitative studies typically select information-rich cases for in-depth
study ‘from which one can learn a great deal about issues of central importance to the
purpose of the research’
(Patton, 1990, p. 169) without making claims to be representative
of a larger population. For the purpose of the PIR, the aim of the stakeholder consultation
was to canvass a range of views and perspectives on the successes and challenges of
implementing the Measure. A further aim of the consultations was to identify any issues
that stakeholders felt should be considered for any impact evaluation of the Measure.
3.4 No Jab, No Pay workshop
The research team facilitated a workshop with 16 stakeholders in DSS National Office in
November 2016. Workshop attendees included a range of participants from the four
departments responsible for policy implementation, including individuals with knowledge of
the relevant databases. The workshop provided the opportunity to present the findings of
the PIR, including the program logic and theory of change, and the preliminary impact
evaluation framework. Workshop attendees were invited to provide feedback on the
material presented, and the research team followed up with a number of staff following the
workshop to clarify issues and source additional documentation.
3.5 Analysis and synthesis of findings
The analysis involved triangulation of data, including the review of policy documentation,
and insights from the data scoping exercise and from the qualitative data collected.
Social Policy Research Centre 2017
22
link to page 95 link to page 95 link to page 94 link to page 94 link to page 94 link to page 94
4 Findings
This section presents the findings of the PIR as they relate to the key research questions.
4.1 Policy Design
The PIR was guided by two key questions with respect to policy design:
•
Has implementation been consistent with the Measure's policy design?
•
If there have been any deviations from the original design, have these been
positive or negative in nature?
To address these questions, we first review the policy design.
Australian Government child care payments (currently called Child Care Benefit (CCB) and
Child Care Rebate (CCR)) have been linked to immunisation status since 1998. Since
2012, payment of Family Tax Benefit (FTB) Part A supplement was also linked to
immunisation status at certain ages. Although these payments were linked to immunisation
status, parents could access CCB, CCR & FTB Part A supplement if they registered a
conscientious objection (CO) to having their child immunised.
On 23 November 2015, the No Jab, No Pay 2015–16 Budget measure was passed in the
Social Services Legislation Amendment (No Jab, No Pay) Act 2015 (Parliament of
Australia, 2015).
The goals of the Measure were to:
•
‘reinforce the importance of immunisation and protecting public health by
strengthening immunisation requirements for children’
(Department of Social
Services, 2016, p. 1)
•
‘amend the immunisation requirements that apply to Australian Government child
care payments and the FTB Part A supplement’.
(Department of Social Services,
2016, p. 1).
While the Measure was expected to save over $500 million over three years, these
savings were not the intended goal of the Measure.
Implementation of the Measure required activation of three separate mechanisms in
addition to other related measures/legislation. The three mechanisms outlined in the
legislation were: a modification of existing exemption categories; extending eligibility
monitoring; and changes to the existing grace period for children who were not up to date
with immunisations. These legislative changes were put into effect through DHS systems.
Associated measures and legislative changes (described further below) were:
•
the expansion of the Australian Childhood Immunisation Register (ACIR);
•
Vaccination Providers who administer and report catch-up vaccinations for children
up to 7 years of age) who are more than two months overdue and who receive all
Social Policy Research Centre 2017
23
link to page 96 link to page 96 link to page 95 link to page 95 link to page 95 link to page 94
scheduled vaccines at that scheduled point (2, 4, 6, 12, 18 months and 4 years of
age) can receive a catch-up notification payment; and
•
free ‘catch-up’ vaccines for individuals aged 10 up to 20 years and who are in
receipt of family payments.
In addition, legislation in New South Wales, Queensland and Victoria introduced ‘No Jab
No Play’ requirements, restricting access to child care centres for children who are not
immunised.
The Australian Government has also proposed phasing out of the FTB Part A end of year
supplement, which would also impact on the No Jab, No Pay measure.
4.1.1 Exemption categories
Prior to the introduction of the Measure, parents could continue to access child care
payments and FTB Part A supplement if their child was not up to date with their
immunisations if the parent completed an
Immunisation exemption conscientious objection
form with a recognised immunisation provider and registered their objection with
ACIR/AIR. Exemptions had also been granted on religious grounds to children of members
of the Church of Christ, Scientist. With the introduction of the Measure, these two
exemption categories were removed. As a result, from 1 January 2016, parents who
registered as conscientious objectors or as members of the Church of Christ, Scientist
were no longer eligible for child care payments and FTB Part A supplement if their child
was not up to date with their immunisations or on a catch-up schedule. Exemptions still
remain for children with a medical contraindication, with natural immunity or who are
participating in a vaccine study
(Senate Community Affairs Legislation Committee, 2015,
pp. 2-3).
The
Social Services Legislation Amendment (No Jab, No Pay) Act 2015 (Parliament of
Australia, 2015) repealed Section 7 of the
A New Tax System (Family Assistance) Act
1999 (Parliament of Australia, 1999) which provided that the ‘Minister may make
determinations in relation to the immunisation requirements’. Instead a new section 6(6)
was included that provides that a child meets the immunisation requirements if the
Secretary determines that the child meets the requirements. The Act provides, in section
6(7) that the Secretary must comply with any decision-making principles set out in a
legislative instrument made by the Minister, for the purposes of that subsection. Currently,
the
Family Assistance (Meeting the Immunisation Requirements) Principles 2015
(Australian Government, 2015b) allow the Secretary to make such a determination
in the
following circumstances:
•
if the child is under 15 years of age, a person with legal authority to make decisions
about the medical treatment of the child has refused, or failed within a reasonable
time to provide consent or, if the child is aged at least 15 years of age, the child has
refused, or failed within a reasonable time, to provide consent to be immunised
•
if
there is a risk of family violence if action is taken to meet immunisation
requirements
Social Policy Research Centre 2017
24
link to page 94
•
if the parent becomes a permanent humanitarian visa holder within 6 months of the
child’s arrival to Australia
•
if the child is vaccinated outside of Australia and certified by a medical practitioner
in respect of the FTB Part A Supplement only
•
if the child is at a heightened risk of serious abuse or neglect if the Secretary does
not make a determination that the child meets the immunisation requirements in
respect of child care payments only.
4.1.2 Eligibility monitoring
Previously eligibility was checked against immunisation requirements at ages 1, 2 and 5
for FTB Part A supplement and each year up to age 7 for child care payments. With the
introduction of the Measure, eligibility for all payments will be checked against
immunisation requirements each year until the child is aged 20 years (Senate Community
Affairs Legislation Committee, 2015: 3).
4.1.3 Changes to the 63 day grace period
Previously, a 63-day grace period was available for children to commence a catch-up
schedule if they did not meet the immunisation requirements when the individual first
attempted to claim child care payments. During this initial grace period, parents could
access child care payments. With the introduction of the Measure, this initial grace period
has been removed for new claimants, and the immunisation requirements must be met in
order for an initial CCB claim to be approved. Grace periods still apply if a child
subsequently stops meeting the requirements, in which case parents are notified and
advised to take steps to bring the child back up to date or risk having child care payments
cancelled.
4.1.4 Other related measures/legislation
Implementation of the Measure also required the introduction of additional measures and
legislative changes. These were: the expansion of the ACIR, ‘catch-up’ notification
payments, and the provision of catch-up vaccines for individuals aged 10 to 20 years of
age for eligible recipients.
Expansion of the Australian [Childhood] Immunisation Register
The expansion of the ACIR was the responsibility of Health. The ACIR, renamed the AIR
from 30 September 2016, was expanded in order to record vaccination information for
people up to 20 years of age in order to facilitate the extension of eligibility monitoring for
payments
(Department of Social Services, 2016, p. 2). The legislative changes were
outlined in the
Australian Immunisation Register Act 2015 and
Australian Immunisation
Register (Consequential and Transitional Provisions) Act 2015.
The
Project Management Plan Extending Immunisation Requirements, Project
Management Framework developed by DHS Services (April 2015) refers to the extension
of the ACIR to include the immunisation records for children up to 20 years. ICT system
changes required were: ‘Full end to end system solution to support implementation of the
Social Policy Research Centre 2017
25
link to page 94 link to page 94 link to page 94 link to page 60 link to page 94 link to page 94
policy change across the Centrelink master programme and Medicare master programme,
as well as datalink between the ACIR and ISIS systems’. From an implementation
perspective, recognised constraints included:
• the existing ICT systems had to be used to deliver the business solutions
• ICT capacity and ICT knowledge of ISIS/ACIR systems could affect the program.
Concerns were expressed about the completeness of ACIR records prior to the
implementation of the Measure in submissions to the Senate Community Affairs
Legislation Committee Inquiry into the
Social Services Legislation Amendment (No Jab, No
Pay) Bill 2015. In terms of the expansion of the register, there were a range of concerns
and issues listed in the issues log relating to data quality, including the software used by
some immunisation providers and cases of Immunisation History Backlog in some states
and territories.
‘Catch-up’ immunisation arrangements
In preparation for the introduction of the Measure, arrangements were made to try to
ensure that children who were incompletely immunised could commence a catch-up
schedule and thereby meet/continue to meet eligibility for CCB, CCR and FTB Part A
Supplement payments. The arrangements included:
• extending eligibility for free National Immunisation Programme (NIP) vaccines to all
children under 10 years of age
• the funding of a new catch-up scheme for children aged 10 to 20 years and the
provision of free vaccines to existing CCB, CCR and FTB Part A recipients
(receiving payments on 31 December 2015). This catch-up scheme is available
until 31 December 2017
(Department of Social Services, 2016, p. 2). A document
outlining the processes involved in extending immunisation requirements to
children over 10 years of age was developed by the DHS
(Australian Government,
2015a).
An NIP information update for vaccination providers produced by Health reported that DHS
would inform families if their child did not meet immunisation requirements for family
assistance payments, and that families would be encouraged to speak to a vaccination
provider about updating their records or commencing a catch-up schedule (see Section
4.6.3). The information update also indicated that Health would provide general
practitioners and other immunisation providers with information about the catch-up
immunisation schedule, how to check a child’s immunisation history, how to order vaccines
and how to update immunisation records in ACIR
(Australian Government, no date). A
factsheet for vaccination providers outlining the new immunisation requirements for family
assistance payments was also developed by Health
(Australian Goverrment, 2015).
Incentive payment scheme for general practitioners and immunisation
providers
Although not part of the Measure, a $26 million measure titled
Improving Immunisation
Coverage Rates was announced in the 2015–16 Budget. This additional funding was used
to fund an incentive payment scheme to encourage general practitioners and other
Social Policy Research Centre 2017
26
link to page 96 link to page 96 link to page 96 link to page 96 link to page 96 link to page 96 link to page 95 link to page 95
immunisation providers to identify and immunise children up to 7 years of age in their
practice who were more than two months overdue for their vaccinations. The $6 incentive
payment was in addition to the existing $6 that vaccination providers receive to deliver the
vaccination. The funding was also used to ‘improv[e] public vaccination records and
reminder systems; greater public awareness of the benefits of vaccinations; and the
Government’s already announced “no jab, no play, no pay’ policy”’
(The Hon Sussan Ley
MP, 2015).
Phasing out of FTB Part A supplement
Legislation was introduced to the House of Representatives seeking to gradually phase out
the FTB Part A supplement by 2018
(Senate Community Affairs Legislation Committee,
2015, p. 3). With the proposed cessation of this payment, it would only operate as a policy
lever to increase vaccination rates in the short-term. This legislation has not yet passed,
however, on 31 August 2016, the Government introduced an income limit for FTB Part A
supplement. From the 2016–17 entitlement year the FTB Part A supplement will be limited
to families with an adjusted taxable income of $80 000 or less
(Parliament of Australia,
2016). However, the Child Care Rebate is not subject to a means test, and as such is likely
to have an impact across all families with children in child care, regardless of family
income.
Related state legislation
Three of the states – New South Wales, Queensland and Victoria – enacted legislation
relating to children’s immunisation status and attendance at childcare and preschool,
known as ‘No Jab, No Play’ policies
(National Centre for Immunisation Research &
Surveillance, 2016). These policies concerned immunisation status and children’s access
to childcare, and had no bearing on their ability to access family payments.
• New South Wales introduced immunisation requirements for enrolment in child
care facilities from 1 January 2014. The legislation allows for conscientious
objectors to still be enrolled, but unvaccinated children can be excluded in the
event of an outbreak of a vaccine-preventable disease.
• Queensland introduced immunisation requirements, ‘No Jab, No Play’, from 1
January 2016 to allow the managers of child care services the option to refuse,
cancel or place a condition on the enrolment or attendance of a child who is not
vaccinated or up to date with the immunisation schedule. There are no exemptions
for conscientious objectors.
• Victoria also introduced immunisation requirements, ‘No Jab, No Play’, from
1 January 2016, which requires children to be fully immunised in order to attend
child care (long day care, occasional care and family day care) and kindergarten
(preschool). There are no exemptions for conscientious objectors, only for those
with medical reasons and for certain disadvantaged and vulnerable children
(including: Aboriginal and Torres Strait Islander children; children who hold a health
care card, whose parents hold a health care card, pensioner concession card, a
Veteran’s Affairs Gold or White card; refugees or asylum seekers; children known
to child protection; children living in emergency or crisis accommodation, or of no
fixed address due to family violence or homelessness; children evacuated due to
Social Policy Research Centre 2017
27
link to page 96 link to page 96
emergency such as flood; or children in emergency care) who are eligible for a
grace period of 16 weeks to meet vaccination requirements
(Victorian Government,
2016).
4.2 Implementation and Policy Design
The PIR set out to assess whether implementation of the Measure has been consistent
with the Measure's policy design.
The document review highlighted how the Measure was designed to ‘reinforce the
importance of immunisation and protecting public health by strengthening immunisation
requirements for children’. This was achieved by linking eligibility for child care and family
payments with a child’s immunisation status through three key mechanisms: removal of
conscientious objection as a valid exemption category; monitoring eligibility for family
payments for children up to 20 years of age; and removing the 63-day initial grace period
for new recipients to get up to date with immunisations for child care payment new claims.
The document review also confirms that implementation was consistent with the Measure's
policy design. Activation of the three mechanisms was supported by the detailed
implementation plans from DSS and DHS, with the latter outlining the expansion of the
ACIR. Implementation was also supported by the complementary measures introduced by
Health.
4.2.1 Policy Implementation
Through the stakeholder consultations, the government stakeholders felt that the
implementation of the Measure had been broadly consistent with the policy’s design. While
the policy had undergone some changes since it was originally conceived, these were
generally carried out before the Measure was launched. A number of challenges arose in
the early implementation stages that required a system response, but these do not
constitute deviations from the policy design.
Most of the external stakeholders felt that the policy’s implementation had been consistent
with the design of the Measure. However, some said that they had not been consulted on
the design in the first place or were unaware of the original design:
I don’t think there was any consideration of how it would affect other people, especially at
state level. A heads up would’ve been nice. You like to think you’re partners, so it’s quite
undermining. It could’ve fallen over if it wasn’t for the good grace of states and territories
and every immunisation provider.
One of the reasons is that there was no prior consultation – we could have told them about
issues that would be a barrier or would not be appropriate.
I’m not objecting to the principles of the Measure but the way it has been implemented and
foisted onto state government people has been outrageous. (ES)
Several external stakeholders also commented on the intent of the policy, viewing it
primarily as a cost-saving measure:
Social Policy Research Centre 2017
28
This is the cynic in me – I think the policy was designed primarily as a money saving
exercise rather than an immunisation coverage exercise. That was a nice side benefit but
that wasn’t the main goal.
So this was a cost saving initiative, targeted at conscientious objectors. (ES)
A key challenge identified by both government and external stakeholders in implementing
the Measure concerned the eight-month timeframe between the policy announcement and
its implementation. The tight timeframe was identified as being particularly challenging for
the staff who had to implement the Measure without additional resourcing. Key
implementation challenges included the associated changes to the ACIR, the uncertainty
around when the legislation would pass and limited timeframes for engaging and
communicating with stakeholders. Both government and external stakeholders commented
that the timing of policy implementation, in January when many families were on holidays,
also added to the implementation challenges.
The greatest issue was the short time frame to implement this. It was quite a big piece of
work. Also we had very limited experienced staff who have the experience to deal with it. In
my team in the project area we weren’t given extra resources. It meant that one or two
people had to do all the work, and work long hours. But it got done and on time. (GS).
There were issues with the legislation – it went to committee which delayed it a bit, so we
were holding our breath waiting for that to be passed, then had to wait for the exemptions to
come through, which came very late. (GS)
The timeframes got a bit too tight, which was very unhelpful. We have a network of over 600
services and we have to communicate the changes to them and it doesn’t help if it’s coming
down to the wire. You’re looking for traction quite quickly and it’s a significant change for
families. It wasn’t a complex policy change, but the admin was complicated and took time.
(ES)
The PIR also set out to assess whether there had been any deviations from the original
design of the Measure and, if so, whether these deviations had been positive or negative
in nature.
The general view from government stakeholders was that any deviations from the original
design were relatively minor and were easily addressed. For example, two stakeholders
mentioned that their perception was that the original design was narrower than what was
subsequently developed, with a different range of ages being affected by the Measure, and
the strict exclusion of non-medical exemptions having to be softened to deal with cases
such as grandparent carers and family violence. Some stakeholders also commented that
the deviations that did occur were either anticipated or relatively easily mitigated through
subsequent actions:
I guess right at the costing time there were probably a couple of variations of the policy that
were debated and considered, but once the policy was agreed to, it’s been implemented
pretty much as envisaged. (GS)
It was mostly just expanding on the existing legislation. It was already a fairly mature policy
that was just being tweaked. (GS)
The document review highlighted two key deviations from the original policy design:
1. The extension of payments beyond the initial grace period for existing recipients
Social Policy Research Centre 2017
29
When the policy was implemented on 1 January 2016, existing recipients whose children
were not up to date with their immunisations were advised that they had entered a 63-day
grace period within which they could commence a catch-up schedule to complete
immunisations and continue to access child care payments. The implementation of the
policy prompted a significant increase in data being uploaded to the ACIR, resulting in
backlogs and delays. There was concern that some recipients could be affected by the
delays and lose their eligibility for child care payments (as FTB Part A is only determined
at the end of the financial year). In response to the data processing delays, the Prime
Minister agreed on 8 March 2016 to pay child care payment recipients past the grace
period end date until 30 April 2016, until the processing delay issue had been resolved,
and raise debts for recipients who were subsequently found to have not met immunisation
requirements at 18 March 2016 (the end of the grace period). This issue was also
identified through the stakeholder consultation:
Around March 2016 it became apparent that the states and territories were experiencing a
high workload processing vaccinations in their own health networks, so there were some
concerns expressed that some parents may have got their children vaccinated but the
provider hadn’t had a chance to lodge the notification, so there was a decision made to
extend payments for childcare customers until the end of April to allow for those
notifications to flow through. (GS)
s47E(d)
s47E(d)
The stakeholder consultation identified further potential issues and process changes that
could be considered, however these are still being finalised. These concerned relaxing the
requirements that only general practitioners (rather than specialists) could approve medical
exemptions, and that children with complex issues that may prevent them from being
immunised (such as the potential for them to self-harm or harm others) may also be
exempted. These could potentially be considered deviations from the original policy
Social Policy Research Centre 2017
30
link to page 96 link to page 96 link to page 96 link to page 96 link to page 96 link to page 95 link to page 95 link to page 95 link to page 95 link to page 96 link to page 96
design, but are effectively refinements, as the proposed changes would still be consistent
with the key policy intentions.
4.2.2 Policy Comment
From a policy design perspective, several submissions to the Senate Community Affairs
Legislation Committee proposed alternative approaches for increasing immunisation rates.
These included:
• addressing structural and practical barriers to immunisation uptake by initiating
home visiting programs
(Public Health Association of Australia, 2015; The Royal
Australasian College of Physicians, 2015)
• developing tools and communication materials to assist immunisation providers to
have conversations with vaccine-hesitant parents
(The Royal Australasian College
of Physicians, 2015)2
• addressing gaps in immunisation provider knowledge through ‘increasing
vaccination training in the medical curriculum’, for example
(Leask & Wiley, 2015,
p. 13)
• engaging Primary Health Networks to play a role in the community
(Leask & Wiley,
2015, p. 13) to implement a program to reduce the incidence of vaccine refusal
using a range of strategies
• implementing a national vaccine reminder system
(The Royal Australasian College
of Physicians, 2015).
It is possible that some of these additional approaches are being considered. For example,
the Victorian Department of Health has developed the
VaxOnTime app to remind parents
about their children’s immunisations. However, none of the documents provided to the
research team could shed light on the development of other complementary measures, nor
was it within scope of this project.
4.2.3 Summary
From a policy implementation perspective, overall, most government stakeholders felt that
the Measure was successfully implemented despite some implementation challenges:
There have been hiccups but by and large the process in place to manage the project and
the implementation has been successful. (GS)
We implemented a measure under difficult conditions despite delays etc. So payments went
out the door when they should to those who needed to be paid and people weren’t paid
when they shouldn’t have been, so it was successful in that sense. (GS)
This is sort of what we do – we implement government measures. It’s been quite full on but
not necessarily out of the ordinary and relatively positively received. We never expect
applause but we hope we don’t get shouted down. (GS)
2 In response, the Australian Government Department of Health funded and produced ‘fast fact sheets’ by a
group of researchers called the SARAH Collaboration on topics including: ‘What is in vaccines?’ ‘How do
vaccines affect immunity?’, ‘Why is the schedule the way it is?’, ‘How are vaccines shown to be safe?’.
Social Policy Research Centre 2017
31
At the same time, many government stakeholders acknowledged that external
stakeholders may not feel as positive about implementation and may have had to do a lot
of extra work without additional resources. This dissatisfaction with the Measure’s
implementation is evident in the external stakeholders’ comments:
We call it ‘No jab no pay, but lots of pain’ …This was the most poorly conceived and
implemented initiative I’ve had anything to do with … Quite a lot of people have been
scarred by no jab no pay. (ES)
This is the most ill-considered policy that I’ve had to be associated with. It’s been absolutely
beyond belief. A dog’s breakfast. (ES)
Implementation of the Measure was consistent with the Measure’s policy design and was
facilitated by the detailed implementation plans from DSS and DHS, and by the
complementary measures introduced by Health. Two key implementation challenges
concerned the need to:
• extend the payments beyond the initial grace period for existing recipients, to
prevent parents from losing access to child care payments when their child’s
immunisations were up to date (due to delays in states/territories updating the
ACIR)
• amend the continuous/rolling catch-up anomaly which could have enabled
parents to delay vaccination indefinitely and continue to receive family
payments.
If not promptly addressed these could have enabled parents to delay vaccination
indefinitely and continue to receive family payments and could have resulted in some
parents losing access to payments even when their child’s immunisations were up to date.
Awareness that the continuous/rolling catch-up scenario could be used to delay
immunisation uptake resulted in efforts to amend the anomaly, which were taken as
quickly as practicable. The data backlog had the potential to adversely affect child care
payment recipients who had managed to get their immunisation records up to date.
However, the extension of the payments beyond the initial 63-day grace period, in addition
to efficiencies in processing the data, appears to have prevented any negative impacts.
Despite these challenges, it appears that implementation did not deviate from the overall
policy design, and in relation to the second point, the change was necessary in order to
maintain the intention of the policy.
4.3 Dealing with issues and risks
With respect to issues and risks, the PIR explored the successes and challenges
(including design, system, data, communications, and uptake of immunisation by the target
populations) that were encountered in implementing the Measure. The DSS NJNP Project
Plan provides the following definitions:
• ‘An issue is an event or set of events that is currently impacting any component of
the project’
• ‘A risk is an uncertain event or set of events that, should it occur, will impact any
component of the project’ (DSS NJNP Project Plan 2015:24).
Social Policy Research Centre 2017
32
link to page 35
4.3.1 Management of issues and risks
A number of policies and procedures were put in place to identify issues and risks that
could negatively affect implementation of the Measure. These included:
• an issues register and a risk log maintained by DSS
• an issues register maintained by DHS
• the working group and IDC, which were also key to identifying, discussing and
strategising to mitigate issues and risks.
DSS risk register & risk log
DSS NJNP Project Plan outlines that the risk register was maintained by the DSS; risks
were managed ‘according to the Risk Management Framework of the Department’, and
were to be directed to the Project Sponsor if escalation was required (DSS NJNP Project
Plan 2015:24). The initial SWOT analysis in the Risk Register identified the internal
environment weakness as ‘the management information to support the success of the
Measure’ and the external threats as follows: ‘the ACIR records are not up to date, class
action before the High Court, vaccine shortages and legislation does not get passed on
time’. Treatments outlined for addressing risks included awareness of appropriate
processes and issues as they arise, and a range of communications strategies with
departments, stakeholders and recipients. The Risk Log categorised risks according to the
criteria in
Table 2 below.
Table 2 No Jab No Pay DSS risk log
Risk
Number and owner
Identify risk:
Risk, risk category (or risk type), sources (what would be the root
cause of this happening?), impacts (what would happen as a result)
Analyse risk:
Current controls (what are we already doing that would help manage
the risk?), are the controls effective?, likelihood, consequence
Evaluate risk:
Risk rating, risk acceptable?
Treat risk:
Treatments (what further action is needed?); who is responsible for
treatment? Implementation timetable (e.g. month, year); likelihood
(after treatment); consequence after treatment; target risk rating (after
treatment); monitor, review and evaluate; Effectiveness of Treatment
Strategies.
Status comments
The DSS Risk Log (July–Aug. 2016) identified nine risks:
1. National immunisation rates fall
2. Unauthorised or inappropriate use or disclosure of information (e.g. transfer of
ACIR information to ISIS)
Social Policy Research Centre 2017
33
3.
Implementation issues arise
4.
Legal challenge to constitutional validity of the Measure
5.
Child suffers adverse reaction and parents try to sue Australian Government
6.
Secretary's Exemptions don't capture all possible categories and some recipients
disadvantaged
7.
Technical amendments to legislation don't pass during desired sittings
8.
Amendments required to National Immunisation Program
9.
Incidence of fraud is identified as a result of Medical Exemptions forms being
tampered with or modified which are accepted by ACIR, which is transferred to
DHS system as meeting immunisation requirements.
Each of these identified risks was categorised and assessed with contingency plans for
addressing the risk outlined in the risk log.
DHS Issues register & issues log
DSS NJNP Project Plan and Working Group minutes (14 May 2015) indicate that the
issues register was maintained by the DHS, who would identify issues that need to be
resolved, and who would also invite stakeholders to provide issues for the register. The
minutes note that:
• where possible, DHS will identify the responsible policy area or areas that will need
to provide resolutions; however, the register will be distributed to all members of
the working group
• issues can be raised by emailing the working group secretariat or within working
group meetings
• where an issue is the responsibility of all policy areas, DSS (Family Payment
Management and Implementation team) will coordinate the combined response.
The Issues Register outlined a wide range of issues, which seem to have been addressed
prior to the implementation of the Measure (including product and payment processing,
communications and refugees), as well as issues raised after 1 January 2016 relating to:
•
policy advice and design issues relating to clarification around the Secretary’s
Exemptions and the processes for determination, review and appeal of decisions
•
payment processing issues relating to categories of children – at risk, children with
disability, timing of payments and immunisation status changes – and whether
exemptions apply.
The DHS Issues Log identified twelve issues, initially raised on the following dates:
1.
The costs of vaccine catch-up schedules for parents with children over 10 years
(18 May 2015)
2.
Exemptions for children vaccinated overseas whose immunisations were unable to
be verified by local immunisation providers (27 May 2015)
3.
Exemptions in the case of risk of family violence (1 June 2015)
4.
Non-parent carers without legal guardianship, where the parent does not allow
vaccines to be given (30 August 2015)
5.
Processes for determining new Secretary’s Exemptions (8 September 2015)
Social Policy Research Centre 2017
34
6. Approval for the communication strategy and impact of delays in passage of
legislation (17 September 2015)
7. Costs of communication strategy and whether it would trigger Government
campaign guidelines (17 September 2015)
8. The negative impact of policy on vaccine objectors (17 September 2015)
9. Data software used by immunisation providers needing to be updated to accept
records of older children (17 September 2015)
10. Delays in passage of Legislation (12 May 2016)
11. Immunisation history backlog processes in the state and territory health
departments (17 February 2016)
12. Fraudulent medical exemption forms received by ACIR – frontline staff being
bullied by parents and some forms may have been processed (14 June 2016).
Working Group & Interdepartmental Committee (IDC) minutes
The Working Group (WG) and Interdepartmental Committee (IDC) were also key to
identifying, discussing and strategising to mitigate issues and risks. Issues identified in the
WG and IDC minutes included:
• delays in uploading information into the ACIR
• delays in obtaining the data software for updating ACIR
• DHS system issues
• vaccine availability
• exemptions
• complex scenarios.
4.3.2 Issues and risks:
This section brings together findings from the document review and the stakeholder
consultation regarding successes and challenges (including design, system, data,
communications, and uptake of immunisation by the target populations) encountered in
implementing the Measure.
Design
Challenges in policy design that were identified in the document review included: a
potential court challenge to the legality of the Measure, coverage of the Secretary
Exemption categories, fraudulent medical exemption forms and eligibility monitoring.
Challenges identified by stakeholders reiterated concerns about exemption categories.
Potential challenge to the legality of the Measure
The Risk Register highlighted concerns that anti-vaxxers would launch a legal challenge to
the constitutional validity of the Measure and indicated that legal advice had been sought
and consultations with departmental stakeholders would continue on this issue. At the IDC
on 16 March 2016, this issue was placed on a watch list for monitoring as one of the
complex scenarios. DSS advised that anti-vaxxers had commenced a campaign
Social Policy Research Centre 2017
35
link to page 94
threatening a class action lawsuit against the Government on the Measure with 700 letters
sent to representatives of the Australian Government, including the Minister for Social
Services and the Hon Christian Porter MP. Despite fundraising to mount a legal challenge
to the legislation, the Australian Vaccination-skeptics Network website reported on 26
December 2016 that they were advised by legal counsel ‘not to proceed due to the poor
chance of success and the high costs of a High Court challenge’3.
Secretary Exemption categories
The Risk Register anticipated that the Secretary’s Exemptions may not cover all possible
categories and some recipients would be inappropriately disadvantaged. Categories of
disadvantaged recipients that were identified prior to the implementation date and were
included in the list of Secretary’s Exemptions included cases in which:
• the person with the care of the child, such as a foster carer, does not have legal
authority to make decisions about the medical treatment of the child, due to not
having consent of the parent to the child being immunised (the child must be in the
care of another individual under a child welfare law for the purposes of the FTB
Part A supplement)
• taking action to meet the immunisation requirements would result in the individual
or the child being at risk of family violence
• the individual is a new permanent humanitarian visa holder and has not had the
opportunity to immunise their child
• the child has been vaccinated overseas, remains outside Australia and the child is
otherwise unable to meet the immunisation requirements, as they are unable to
have a recognised immunisation provider certify that the child has received the
same level of immunisation overseas (FTB only)
• the child is at risk (CCB only)
(Australian Government, 2016b).
Prior to the implementation date, issues were raised about determination processes for
eligibility for Secretary Exemptions and transferability of exemptions between carers of
children. In both instances, clarification was provided prior to implementation. After 1
January 2016, however, two potential additional categories that were not anticipated or
included in the list of Secretary’s Exemptions included: children having a disruptive
behavioural or developmental disorder; and reduction of the age of consent for a child to
refuse to be vaccinated from 15 to 14, to ensure consistency with state and territory
arrangements for consent to medical procedures (Policy issues register 105 11/1/2016).
With regard to children with severe disability, it was recorded at the IDC on 2 June 2016
that draft amendments had been developed, which were with Health for approval from the
Commonwealth Chief Medical Officer before progressing further.
Two external stakeholders commented on the difficulties around defining legitimate
exemptions. One referred to cases where a child has extreme needle phobia, or where
children have previously had an adverse reaction to immunisation. Whilst acknowledging
that these types of situations can be rare, this stakeholder felt that there was no clear
3 https://avn.org.au/2016/12/bad-news-legal-challenge-front-will-never-give-fight/, viewed 21/02/17.
Social Policy Research Centre 2017
36
communication about what to do or how to appeal for exemption in these kinds of unusual
cases. This stakeholder reported that the lack of clarity around how to manage these kinds
of situations contrasts with other countries’ formalised processes:
When people are genuinely doing the right thing, there should then be absolutely a pathway
for them to have a formalized causality assessment and then having some sort of
compensation redress. That exists in every other major English-speaking developed country
in the world and wasn’t contemplated here (despite being advocated in the Senate
hearings). It’s clearly an obligation to have that in place. (ES)
A government stakeholder also felt that certain non-medical reasons for seeking
exemption, such as children with autism or needle-phobia, had not been adequately
considered:
Some people can’t be immunised because they might be severely autistic, for example, or
very violent with regard to needles; but it’s not an actual medical exemption. Things like that
that we didn’t necessarily cater for or anticipate or give enough thought to. (GS)
Medical Exemption forms
The Risk Log identified concerns about fraud as a result of Medical Exemption forms being
tampered with or modified. At the Working Group meeting 14 June ACIR raised concerns
about ‘a number of suspect medical exemption forms’ provided by a Victorian GP. An
additional box had been inserted on the medical exemption form, indicating exemption
‘until vaccines are proven to be safe by clinical studies …’. The Issues Log on 14 June
additionally noted that ‘Front line staff have been bul ied by parents, and some forms have
been processed (and exemptions may have been given)’. DSS subsequently gave
direction that these fraudulent exemptions forms were not valid and should not be
processed. At the Working Group meeting on 13 July 2016, DHS advised that modified
medical exemption forms were being lodged but were not being processed and were being
returned to providers with a letter from ACIR advising they were not valid. DHS suggested
that Health should consider undertaking further communication to inform vaccination
providers on this issue. Further discussions after July 2016 were to be held in the Working
Group and IDC regarding actions to be taken on this issue.
Eligibility monitoring
The primary issue with eligibility monitoring related to the accuracy of the ACIR data and
delays in processing the data, as discussed further below.
System
The document review identified system challenges concerning Australian Government and
state/territory interactions and vaccine availability. The former is largely concerned with
delays in the states and territories uploading information to the ACIR, which is discussed
below in the section on data. The external stakeholders reported concerns about increased
workloads and financial costs for providers as a result of the Measure.
In terms of successes, the document review identified system responsiveness and
identification and management of complex scenarios as important elements.
Social Policy Research Centre 2017
37
Vaccine availability
Health had the responsibility to report to the IDC on vaccine availability. The only potential
reported shortage identified in the IDC Minutes (29 April 2016) was the Pertussis vaccine.
The shortage did not eventuate and no further action was required.
Workloads and costs
The external stakeholders commented at length about how state-based services, including
local councils, public health units and vaccination providers, had been overwhelmed by the
increased workload that was associated with the implementation of the Measure. On top of
their usual workloads, vaccination providers had to respond to parents’ requests for:
children’s vaccination histories, ensuring that vaccination records were up to date; the
development of catch-up schedules for incompletely immunised children; and the
recording of overseas vaccination histories.
Providers …were floundering and not really coping. Our public health units have had an
immeasurable increase in demand. So a lot of their normal routine work had to be put on
hold. (ES)
You then have this influx of parents needing their vaccine history records put on the register
and they were asking GPs to do it and they’d send it to us but it isn’t our job (nor GPs’ jobs),
so the parents were like ‘Who’s going to do it?’, so the GPs sent the parents to local
councils, who were being inundated with al of these vaccine histories and they couldn’t deal
with it. (ES)
This increased administrative workload came at significant financial cost to some
providers:
We only receive the $6 from ACIR for every reported vaccine that’s given within the correct
schedule. We got that for children caught up under 10, but not for catch-ups for those aged
10-19. And there were nursing costs as well, which is often involved as well. So we were
out of pocket because we have no way of covering the costs of administering the program.
(ES)
A number of the stakeholders also referred to the strain that the implementation put on
supplies of vaccines, with some vaccines running low and having to be sourced from other
programs:
With a program of this nature we weren’t able to determine how much vaccine we would
need because we didn’t know how many people would take it up. So if the vaccine
providers don’t have a forecast they run out of supply. We’ve had to take vaccines from our
national program because people’s payments are being withheld because their kid can’t get
the vaccine from the GP, so we take it from our other supply from the hospitals and send it
to the GPs. (ES)
We had issues trying to source vaccines – some of the vaccines ran low and we had to
juggle supplies which has put a lot of pressure on our routine vaccine distribution system,
so that’s added a lot of financial cost for us too. (ES)
[The Australian Government] provided statements about which vaccines need to be
provided but they didn’t check stocks of these vaccines beforehand. (ES)
Social Policy Research Centre 2017
38
DHS system issues
A key system success relates to system responsiveness when issues were identified. The
14 January 2016 working group minutes note that two key issues were identified by DHS
as likely to have an impact on recipients. s47E(d)
The second issue affected 512 child care
payment recipients who were not placed on the 63-day grace period and whose payments
were affected, with 60 having their payment cancelled. DHS advised that only one
recipient had contacted the department about the issue. When the issue was resolved it
would contact all affected recipients.
The Project status report December 2015–February 2016 notes that a system glitch in
early January 2016 affected less than 5 per cent of the FTB population (approximately
73,000 recipients). s47E(d)
. Another glitch in early January resulted
in approximately 500 Child Care recipients not being placed on the 63-day grace period
before child care payments began to be affected. Both system issues were promptly
addressed by DHS and there was no financial impact on the affected recipients.
Other ‘complex scenarios’
A working group, comprising staff from DHS, DET, Health, and DSS, was formed to
consider options for ‘complex scenarios’ that could affect the implementation of the
Measure. The minutes of the 16 March 2016 IDC meeting documents a range of complex
scenarios that had been discussed by the working group and IDC members at a meeting
on 1 March 2016. The complex scenarios were categorised into three groups:
• those requiring active monitoring
• those placed on a watch list for monitoring
• matters not likely to cause concern at this stage.
Other complex scenarios not discussed elsewhere and categorised as requiring active
monitoring were:
• the impact of ACIR backlog on new recipients; DHS advised that no complaints in
respect of child care payments had been received. Separate discussions on finding
a solution to this issue were being held between relevant agencies
• translating services; members agreed that Health and DHS should work together to
develop possible treatment to resolve the difficulties in having immunisation
documentation translated to enable vaccination providers to update ACIR records
• medical exemptions; Health was exploring options to enable specialist
immunologists and paediatricians to sign medical exemptions
Social Policy Research Centre 2017
39
• catch-up schedules to meet immunisation requirements in ACIR; Health and DHS
were discussing the issue with states and territories, and immunisation software
providers respectively.
On 27 May 2016 the complex scenarios Working Group undertook a stocktake of the
current status of each scenario. Complex scenarios assessed as requiring active
management included:
• medical exemptions; legislation proposals have been completed and are awaiting
authority by the incoming government
• catch-up schedules to meet immunisation requirements in ACIR; immunisation
software provider, Best Practice, has advised ACIR that an updated product
release is imminent.
Data
The document review identified concerns being raised prior to implementation of the
Measure about the quality of the data in the ACIR, delays in uploading data and the ability
to monitor conscientious/vaccination objection.
The government stakeholders most commonly cited issues also relating to updating the
ACIR, particularly in relation to the quality of the existing data and the data provided by
vaccination providers and general practitioners; the expansion of the register to include
children up to 20 years of age; the requirement for parents to update their children’s past
vaccination information; and the alignment of data systems.
Delays in updating ACIR
The Risk Register noted that implementation issues could arise which could influence the
processing of records, resulting in impacts on payments. It rated this risk as almost certain
but with low anticipated impact.
The issue of the Immunisation History Backlog was noted in the Issues Log on 17
February, with advice provided by Health that there was a substantial backlog of
processing of immunisation histories developing in state and territory health departments.
Health has been advised by some jurisdictions that the backlog could not be uploaded into
the ACIR before the end of the child care payments’ 63-day grace period. This could mean
that recipients who had done the right thing and had their child immunised would have
their payments impacted due to the administrative issue.
This issue was raised at the IDC
Extraordinary teleconference 19 February where
‘members agreed to develop a paper to assess viable options for consideration by lead
agency Group Managers. It was agreed that PM&C and Treasury be involved in this
process’.
The Project status report December 2015–February 2016 notes that this backlog was not
likely to affect FTB recipients, as FTB Part A supplement is paid at reconciliation (from 1
July onwards), but would affect child care payment recipients. Health advised that some
jurisdictions could not provide assurance that the backlog of immunisation history
Social Policy Research Centre 2017
40
information could be uploaded into the ACIR system prior to 18 March 2016, which was
the end of the 63-day grace period for current recipients of child care payments.
Consequently, the Prime Minister agreed on 8 March to pay child care payment recipients
past the grace period end date until 30 April, until the processing delay issue had been
resolved, and raise debts for recipients who were subsequently found to have not met
immunisation requirements at 18 March 2016.
Minutes from the 7 April meeting of the IDC note that Health advised that states and
territories continue to be confident that actions within the control of the jurisdictional Public
Health Units were being met, to enable immunisation records to be uploaded as soon as
possible. In addition, Health had signed agreements with selected Primary Health
Networks to assist refugee organisations to translate and update immunisation records.
Minutes from the 29 April meeting of the IDC noted that the processing delay issue had
been largely resolved, with jurisdictions indicating that the accumulation should be cleared
by 30 April. The minutes also noted that support had been provided by Health to Primary
Health Networks in South Australia, Tasmania and Central Queensland to assist in
interpreting and translating records, and to develop catch-up schedules.
The Project status report for March–April 2016 noted that Health advised that state and
territory Health Departments had been progressing well, and the majority of immunisation
history information had been transferred into the ACIR.
A number of issues regarding the ACIR data and processes were raised by the
stakeholders, which provide further insights to the data challenges in implementing the
Measure. A stakeholder reported that the tight timeframe for implementing the Measure
meant that there was not enough time to access the required data to estimate the number
of people who were immunised:
So we went back to publicly available data and fitted that to our purpose, which was to get
an idea of how many people weren’t immunised, which was quite a process. It was the best
data we could get our hands on. We have the benefit of being able to access admin data.
We like to think of that as being close to a perfect data set. (GS)
This stakeholder also pointed out potential issues with the quality of the existing ACIR data
and raised concerns about data linkage with DHS payments systems data.
Another stakeholder also mentioned that poor quality data was provided by some health
providers, further complicating the updating of the ACIR.
Also on one hand we got a lot of good data, but [health providers] have also sent us a lot of
rubbish data, duplicates and so on, because they didn’t understand what we needed and
what was required, so they’d send us data we already had, for example, and there was a lot
of manual intervention to fix that up. From their side they’re probably saying we have a
backlog and haven’t processed it, but we’re saying they sent a lot of rubbish data or
incorrectly reported the numbers of vaccines that had been given. (GS)
Other stakeholders pointed out the challenges that had been presented by the expansion
of the ACIR to include older children and the retrospective requirements to register
vaccinations. Some spoke of missing immunisations for some children, which was
attributed to a variety of possible factors, including doctors not updating immunisation
records, ACIR malfunctions and DHS operator errors. Others spoke of the challenges that
Social Policy Research Centre 2017
41
many parents of older children faced in trying to locate their children’s immunisation
records. This was noted as a particular challenge for older children who had migrated to
Australia several years prior:
Refugees and immigrants … if they came to Australia after 7 years old we didn’t have the
data on the ACIR … so there were massive backlogs and they all had to wait until they were
recorded so they could receive their payments. It was also very hard to interpret data from
foreign databases and sources and then they have to be put on catch-up programs, so
there were backlogs in practices and other community centres and community health
centres. (GS)
The external stakeholders echoed these concerns about the complications involved with
updating records on the ACIR, as well as issues arising from missing and incomplete data.
Concerns about data quality and data linkages between the ACIR and the Centrelink
payment system were considered particularly pertinent when access to financial payments
was at stake.
Parents were being told that their payment was at risk but no information was given to them
about what vaccines they lacked, so there was no start point apart from looking at the
register and trying to work it out. Very few were simple cases who had never had their kids
vaccinated. Quite often they had no knowledge that their register wasn’t complete. (ES)
The biggest issue was trying to assist people with their child’s vaccination records. We have
a state register here too which not all states do. Individual providers with electronic software
send info that goes to the ACIR and [state] database, but the [state] database collects a lot
more info. The NJNP was related to children over 10 but our register only went up to 10,
and also the two registers don’t align in al areas. So it was very complex. We didn’t have
time to think through or plan all this so we’re playing catch-up and a lot of kids are getting
additional vaccines because there’s no record. (ES)
Some government stakeholders pointed out other unforeseen complications in requiring
older children to have their vaccinations registered on the ACIR. Unanticipated challenges
included the fact that privacy laws prevented parents from accessing their children’s
immunisation records if they were over 14 years; and free vaccines were not available to
older children over 10 years if they were a new recipient.
So we had to give these 14–20 year olds the ability to access their own records, after which
their parents could access the records. (GS)
There’s an issue with older children if they’ve missed vaccines. If you’re a new customer
from 1 January you can’t access free vaccines. So if your child is older than 10 you now
need to pay for it. (GS)
It only incentivises families for kids getting family payments. There might be an opportunity
to continue funding for that free vaccine program for 10–20 year olds. (GS)
In spite of the many challenges identified by stakeholders, both government and external
stakeholders pointed to the positive effect the Measure had on updating the ACIR and on
improving data quality:
By extending the ACIR up to 20 years old, it gives a more comprehensive view of the
immunisation records. So people are more up to date, data gaps are fewer, and so on. (GS)
When the system change was made on the 1st of January there were a few glitches but
nothing like the Census. (GS)
Social Policy Research Centre 2017
42
At its heart the policy is aiming to increase rates and accurate reporting of immunisation
coverage and provide accurate data on the proportion of people protected from disease. So
it’s been a very positive outcome in driving public and providers to ensure that the register
data is improved. (ES)
Monitoring conscientious objection
One of the three mechanisms of the Measure was the removal of conscientious objection
as a valid reason for seeking exemption from vaccination. In removing this exemption
category from the ACIR, concerns had been expressed in the Senate inquiry that
implementation of the Measure would remove the ability to track rates of conscientious
objection (now referred to as ‘vaccination objection’). This was echoed by both government
and external stakeholders, who expressed concern that it would no longer be possible to
track this group. One stakeholder thought that this group would be become ‘silent’
conscientious objectors, whilst another expected that the number of medical exemptions
would increase:
You used to be able to measure conscientious objectors but now you can’t measure it – we
want to measure how many people have never had any jabs. They’re probably gonna
become ‘silent conscientious objectors’ and because they’re not claiming payments they’re
now under the radar. (GS)
I’d measure medical exemptions – have those numbers changed? I think a lot of people in
the past may have been recorded as conscientious objectors instead of medical exemptions
by the providers, incorrectly. (GS)
The ability to see who was actually a conscientious objector has been lost. There should
still be a capacity to have some understanding of why people are not up to date. The
register needs to reflect things like whether people have left the country too. We really don’t
know where the gaps in coverage are. (ES)
One government stakeholder made reference to this loss of data and reported that they
had had to come up with a workaround to be able to track conscientious objectors:
So we worked with DHS and [DET] to come up with a solution: we took snapshots of our
customers before January 1 on conscientious objector status because we can’t track them
through the ACIR anymore. (GS)
The minutes from the 15 December 2015 IDC meeting note the Senate Inquiry’s
recommendation that a paper be developed at Working Group level on agreed proxies and
principles for monitoring ‘conscientious objection’. The IDC agreed that the Government
investigate a means of continuing to monitor conscientious objection if the Bill is passed.
Health advised that the New South Wales Government was developing its own
conscientious objection form, which would allow parents to enrol their child in child care
centres. This highlighted how the differing policies and approaches in regard to
immunisation requirements and child care centres by individual states and territories was
an issue of concern. However, only medical exemptions approved by the Australian
Government would be acceptable for child care benefit purposes. Conflicting jurisdictional
requirements were noted as likely to lead to parent confusion.
Other government stakeholders pointed out that the ‘conscientious objector’ statistics from
ACIR could never be considered a comprehensive picture. There was not a requirement to
Social Policy Research Centre 2017
43
link to page 55
‘register’ as a ‘conscientious objector,’ and was only there to enable people to access
linked payments.
Communications
Communication strategies and activities for the Measure are described at length in
Section
4.6. Internal communications for the Measure included interdepartmental
communication around governance and implementation issues, communication with
relevant Ministers’ offices, and communication to departmental staff, who would be dealing
with recipients and would be required to provide the correct information. Key target
audiences for external communications were: parents, vaccination providers and third
parties, including community organisations, child care providers, education and training
providers, and software vendors.
In the document review, the Risk Register identified effective internal and external
communication strategies as a corrective action for a number of the risks identified. The
Issues Log identified two internal issues on 17 September 2015:
• that the ‘communications strategy stil to be approved and delays in implementation
due to legislation may impact on communication activities’. This issue was resolved
and the communications strategy approved.
• the Communications Advice Branch (CAB) in the Department of Finance had
advised that paid advertising on Facebook may trigger the Australian Government
campaign guidelines because the spend may exceed $50,000. This issue was
resolved and the communications strategy approved.
The main challenges about communication that were identified by stakeholders related to
external communications.
The external stakeholders were particularly unhappy with the lack of consultation from
government departments about the impending implementation of the Measure. Many felt
that they were not provided with adequate or timely information to enable them to brief
both immunisation providers and the public about how the Measure would affect them.
It’s been one of the most difficult things we’ve ever had to implement. Our role with the little
information that we were given was to let immunisation providers know and communicate to
members of the public, and also feedback up to the Commonwealth what we needed. (ES)
First we heard about it was about 16 months ago, a teleconference on 8 May with the
Department of Health that it was happening – no asking us before or consultation, just that it
was happening. We had no idea basically. We didn’t really know for a number of months
what our role was or what we had to do. It was hard to prepare our people without having
enough information. So doing that communication was very difficult. (ES)
One external stakeholder contrasted the implementation of the Measure with the
Victorian’s government’s implementation of a similar measure, which the stakeholder felt
was far better managed: ‘They had really comprehensive information and processes. The
implementation was very good. We were very well consulted leading into that’.
Social Policy Research Centre 2017
44
link to page 96 link to page 96
Uptake of immunisation by the target populations
Both government and external stakeholders highlighted some of the successes of the
Measure. Some government stakeholders focussed on the short-term outcomes of the
Measure, such as having raised awareness of immunisation in general, as well as an
overall increase in immunisation rates. ‘We’ve made people change their behaviour – we
may have targeted the conscientious objectors, but recalcitrant parents have [also] gone
out and got their children vaccines.’ (GS)
A media release from the Hon Christian Porter MP, Minister for Social Services, on 6
November 2016 states that ‘[s]ince the last quarter, an additional 39,369 children who
were not fully immunised at 31 December 2015 now meet immunisation requirements
across Australia. This takes to187,695 the number of children now meeting immunisation
requirements who weren’t up to date with their immunisations at the launch of the Measure
on 1 January this year.’
(Porter, 2016b). It is unclear whether these figures reflect a
response to the Measure, whether they are significantly greater than they would have been
without the Measure or whether they are reflective of general trends in immunisation
uptake that would occur over the usual course of a year.
One of the key issues was whether vaccine objectors would change their behaviour in
response to the Measure. Historical ACIR figures show that the percentage of children with
a conscientious objection recorded increased each year between 1999 and 2014 from 0.23
per cent in 1999 to 1.77 per cent in 2014. Between 31 December 2014 and 31 December
2015, the percentage of children with a conscientious objection recorded declined for the
first time, from 1.77 per cent to 1.34 per cent
(http://www.immunise.health.gov.au/internet/immunise/publishing.nsf/Content/acir-cons-
object-hist.htm viewed, 11/11/16). It is possible that some of this decline in 2015 could be
a response to the announcement of the proposed Measure, however, this cannot be stated
categorically as there were several other measures that may have influenced immunisation
uptake, including measures undertaken by Health.
A media release from the Hon Christian Porter MP, Minister for Social Services, on 31 July
2016 states that ‘[m]ore than 5,738 children whose parents are receiving child care
payments and were previously registered as vaccination objectors have had their child/ren
immunised since the launch of the Government’s No Jab, No Pay policy’
(Porter, 2016a). It
is unclear whether these figures reflect a response to the Measure, whether they are
significantly greater than they would have been without the Measure or whether they are
reflective of general trends in immunisation uptake that would occur over the usual course
of a year.
External stakeholders agreed that families from disadvantaged backgrounds and those
who had inadvertently fallen behind with their immunisations may have been motivated to
complete their children’s vaccines as a result of the Measure.
We have a large number of low SES families and we found that a lot of people don’t
complete their schedule not because they object or any principled reason, just because it’s
difficult to make appointments or attend any health service, especially when mental health
issues or drug issues are added. So these latter people were often suitably motivated to get
their kids vaccinated, which was great. (ES)
Social Policy Research Centre 2017
45
link to page 96
It has given people that bit of incentive to get back on track where they’ve fallen behind, or
tip people over who have been on the borderline. (ES)
External stakeholders also felt that, despite the difficulties they had encountered during
implementation, the Measure had appeared to improve immunisation rates.
Our report in June shows that our percentage coverage has gone up; but I don’t know if we
can attribute that to this policy. (ES)
Going on the data that’s been released by the Commonwealth, it does look like there’s been
improvements in rates, especially in the ‘catch-up’ community. (ES)
Eligibility for CCB and FTB payments
Against these successes there were also concerns raised in submissions to the Senate
Inquiry that the policy could have unintended negative consequences on some payment
recipients losing eligibility, particularly low income families and other families who may face
barriers to vaccination
(Senate Community Affairs Legislation Committee, 2015:15). To
date, publically released data from DSS includes Ministerial media releases as well as
data published in the DSS 2015-16 Annual Report. Data on post implementation impact
from the IDC and Working Group minutes show the following:
Eligibility for Child Care Benefit (CCB) recipients:
• on 1 January, 140 000 CCB recipients were to be sent advice that they had entered
the 63-day grace period (WG 15 December 2015). DHS advised that as at 25
March 2016 there were 40 000 CCB recipients with at least one child in a grace
period, including 7 300 former conscientious objectors (IDC, 31 March 2016). This
appears to reflect a substantial decrease in the number of recipients in a grace
period in a relatively short timeframe
• on 2 May 2016, a total of 48 160 recipients had their child care payments
reassessed, and lost eligibility for one or more children in their care who had not
met the immunisation requirements. Of these, 24 059 had child care attendance
recorded since 1 January 2016 and therefore had an immediate cancellation or
reduction in their child care payments. Up to approximately 19 000 recipients may
be issued with a debt as a result of payments extended to 30 April 2016. This work
is scheduled to be undertaken on 23 July 2016 (IDC 2 June 2016).
Eligibility for FTB-A supplement payments from IDC (2 June 2016):
• the latest FTB reminder mail-out had taken place from 16 to 27 May 2016 with 304
301 letters sent to FTB recipients at risk of losing their FTB Part A supplement
payment for 2015–16 if immunisation requirements were not brought up to date
• information was now available to support a snapshot based on known
immunisation status for Family Tax Benefit recipients
• of the approximately 3 million children, DHS expected that 2.5 million would attract
a full-year FTB Part A supplement payment, as they would have met immunisation
requirements. Approximately 31 000 (predominantly 1, 2 and 5 year olds) were
Social Policy Research Centre 2017
46
expected to have their full supplement payment withheld, as they would not have
met immunisation requirements for the full financial year, and approximately 302
000 were expected to receive a part-year supplement payment as the had not met
immunisation requirements, but were not subject to these requirements prior to 1
January 2016.
Two additional factors should be noted regarding these numbers of families whose
eligibility may be affected: the figures for 2016–17 may be lower as the income limit for
FTB Part A Supplement is $80 000 from 2016–17 and recipients have a year after the end
of the financial year to meet reconciliation conditions. The issue of loss of eligibility for
payments, and whether there were any unintended consequences relating to
disadvantaged families losing payments, should be explored in the Impact Review.
4.3.3 Summary
Effective policies and procedures were established to identify issues and risks that could
negatively affect implementation of the Measure. In the first six months of implementation,
several challenges that could potentially derail the smooth implementation of the Measure
were identified. s47E(d)
Actions were promptly taken to minimise impact. An identified
risk/issue that does not appear to have been adequately resolved concerns the loss of
ability to track conscientious objectors.
4.4 Governance
This component of the PIR explored whether governance and decision-making
mechanisms helped or hindered the successful implementation of the Measure.
The governance structure established for the Measure included a high level
Interdepartmental Committee (IDC) and a Working Group to handle practical
implementation issues. These were in addition to the ‘business as usual’ governance
arrangements in each agency. The Working Group and the IDC met on a regular basis,
with the Working Group meeting fortnightly prior to implementation, and monthly post-
implementation. The IDC met monthly, although extraordinary meetings were held as
required (DSS Evaluation Background Summary 2016:2). There was also a separate
Communications sub-committee, as well as some department-specific steering
committees. The IDC will continue to meet until the impact evaluation is completed with
meetings held quarterly. The Working Group will also continue while the IDC exists.
Social Policy Research Centre 2017
47
link to page 35
4.4.1 Interdepartmental Committee (IDC)
The Interdepartmental Committee (IDC) had as its membership senior executives from the
four agencies responsible for implementation of the Measure – DSS, DHS, Health, DET –
as well as representatives from the Departments of Finance, Treasury and the Prime
Minister and Cabinet. The IDC first met in September 2015 and has met every six to eight
weeks or as required, with the most recent meeting held on 14 September 2016. The
terms of reference for the IDC were to inform the development of the Measure by:
•
facilitating cross-agency engagement to ensure all relevant agencies are aware of
their responsibilities in progressing work to support the comeback
•
establishing a forum for issues resolution, change of management and risk
management for issues that arise in the implementation and communications
working groups4
•
providing oversight and guidance to the Working Group for the implementation of
the initiative; guidance may also be sought from the Ministers as required
•
providing oversight and guidance on communication and media strategies around
implementation of the Measure
•
working with key stakeholders involved in implementing the Measure to ensure the
delivery of intended outcomes.
4.4.2 Extending Immunisation Requirements (Immunisation) Working
group
The Working Group includes staff from the four line agencies, with representation from a
range of areas within each agency, such as communications, data, the ACIR and various
functions within DHS. The Working Group commenced meeting in May 2015 and met
every 2–3 weeks through 2015 and 2016. The working group was chaired by DSS with
documentation to be maintained by various Departments listed in the Working
Arrangements documents. The Working Group was responsible for managing the practical
side of the implementation of the Measure. Its purpose was ‘to identify, discuss and where
possible resolve policy, legislative, systems, budgetary or communications issues in
relation to the implementation of the new immunisation requirements and the catch-up
program’ (EIR Working Group - Working Arrangements:1). Where appropriate, the
Working Group was expected to escalate issues to the Immunisation Steering committee
(later known as the No Jab, No Pay IDC).
As noted in the Issues and Risks section (Sectio
n 4.3.1), the IDC and Working Group were
the key to identifying, discussing and strategising to mitigate issues and risks that might
negatively affect implementation of the Measure.
4 Communication from departmental staff indicates that the communications working group was not a formal
working group and it met on an ad hoc basis.
Social Policy Research Centre 2017
48
Stakeholder perspectives
The stakeholder consultations offer some perspectives on the Measure’s governance
arrangements.
The government stakeholders generally agreed that the IDC and Working Group had been
effective and helped the implementation of the Measure. Stakeholders praised the
composition of the groups, the regularity with which they met, and their effective
processes:
All the relevant people from the policy departments attended and made it a priority. People
responded quickly when we needed them to. (GS)
They certainly helped. In such a complicated space, the governance worked well. The two
groups had very different remits, but to get such a big thing implemented in such a short
period of time was due to having all those senior people driving action and meeting
regularly. (GS)
On the steering group there were a lot of very senior staff from across agencies, so it was
good for everyone to touch base and put their cards on the table and say what they could or
couldn’t do. Things that were ‘impossible’ sometimes became possible. (GS)
Several government stakeholders noted the effectiveness of having a single department,
DSS, as the lead department, given that multiple departments and stakeholders were
involved in implementing the Measure. DSS were able to act as a central point of contact
as well as drive the governance actions around implementation. ‘
DSS is always highly responsive and focussed on the task and threw a lot of resources at
the task.’ (GS)
Whilst having DSS as the lead agency was regarded as an efficient arrangement, some
stakeholders felt that this arrangement had its challenges when some departments were
overlooked or particular issues were not considered a priority:
So sometimes it worked well with DSS as the lead and other times we were an afterthought
or decisions were made without consideration for [our department], so we might’ve had to
go back and revisit things, or had no choice in the matter. (GS)
It would be good to look at how the different agencies work together. From an administrative
point of view, that’s where things could’ve been easier, in terms of the way different
agencies interact and communicate with each other. With DSS working in the coordinating
role for this measure it means that we need to rely on them but they may think certain things
are ‘optional’. (GS)
This stakeholder referred to the extension of payments beyond the initial grace period due
to the delays in uploading data to the ACIR as an example of how the governance
arrangements could complicate the decision-making process:
The IDC’s involvement in this slowed the process because of the number of meetings
necessary. They didn’t make a quick decision and action it. Everyone had to see the letter
that would go out to families. The way it was handled caused a lot of heartache for a lot of
people. DSS and other departments probably had more input into the outcome than I felt it
should have, so it was something that probably could’ve been knocked on the head in a
couple of weeks, but instead it took months and had to go to the PM before a decision was
made. (GS)
Social Policy Research Centre 2017
49
The external stakeholders did not feel that the governance structures ensured that they
were adequately informed of how implementation of the Measure was likely to affect them,
nor did they feel that their concerns had been acknowledged:
We got certain information but it was very infrequent and coming in statement form that told
us the big picture but didn’t help us with any of the complexities of program delivery. Even
basic information like ‘we’ve sent x number of letters to clients in your state or council area’,
which would have given us a heads up to the volume of demand coming our way. (ES)
When we were highlighting our concerns about the implementation, I felt that it didn’t matter
how many difficulties this program was going to create, or how much it hurt disadvantaged
people, there was no way the policy was going to be stopped, regardless of how badly it
was implemented, and I thought that was so wrong. (ES)
Additionally, some external stakeholders felt that the governance arrangements for
implementing the Measure, with DSS as the lead agency, made the implementation
process all the more difficult for health providers who were more accustomed to dealing
with Health. There was a sense that DSS did not have an adequate understanding of ‘on
the ground’ implementation issues for what was considered to be a health initiative.
Normally our interaction is with the Department of Health but this was with DSS. That
caused some issues in that we don’t see communications between departments and it
seemed that DoH people were in the middle and put in a difficult situation. It had significant
implications for state and territory public health units and immunisation providers but there
were no opportunities to go back ‘direct to source’ to DSS but rather through DoH. (ES)
It’s run out of two branches of DSS and DHS and it’s really a health initiative. I find there’s a
disconnect. DHS are not charged with delivering health preventative measures. So having it
run out of them has posed difficulties. There may be broader strategic and governance
issues around what is the overarching aim of the policy which needs to be addressed by a
high level governance or advisory group that can advise both branches of government. This
is not a DHS measure at its core – it’s about people’s health. (ES)
4.4.3 Summary
The successful implementation of the Measure was bolstered by the establishment of
effective governance structures at a range of levels, with the higher level Interdepartmental
Committee (IDC) and a Working Group, ongoing governance structures in each
department, and a communications sub-committee. These structures were effective in
identifying and strategising to mitigate issues and risks.
4.5 Service delivery
The review examined whether the service delivery model resulted in impacted recipients
having positive or negative encounters. The documents reviewed provided little insight into
service delivery, however the stakeholder consultation did.
Government stakeholders and external stakeholders were asked about the impact of the
Measure on targeted recipients, and whether recipients’ experiences were generally
positive or negative. Most government stakeholders felt that impacted recipients had had a
positive experience with the new requirements. This was largely attributed to the public’s
acceptance of the overall aims of the Measure.
Social Policy Research Centre 2017
50
As a whole the general public seem to be really accepting of the Measure and think it’s a
good idea. (GS)
Because I think the general community response to the policy has been positive and by and
large the majority of the community is supportive of increasing the vaccination rates and as
such don’t have any problems tying it to receipt of payments. Most customers meet the
requirements so aren’t negatively affected. (GS)
Hopefully the majority have had a positive experience meeting the requirements as we’ve
tried to make it as painless as we can, but when you’re dealing with mil ions of people not
everyone will have a smooth experience. (GS)
Government stakeholders nominated two areas in which recipients’ experiences were
negative. Firstly, there was some confusion for recipients around the process of updating
their children’s vaccination details in ACIR, as well as delays for some recipients in having
their records updated due to data bottlenecks and issues with the link between the ACIR
and Centrelink databases.
There’s been some noise around the actual process to get your records updated and how
long that takes, and the admin process between Centrelink and the [ACIR]. (GS)
There might’ve been a lot of frustration from those who may have been up to date but got a
letter saying they weren’t up to date. They would cal us and ask why the records weren’t
sent to Centrelink but we need some sort of trigger mechanism to give us authorization for
us to establish that link. Centrelink don’t know if parents are up to date – we have to provide
that record to them. (GS)
Depends on the payment. For FTB customers, targeting the older cohorts, there was a lot of
confusion and people were rushing to get their kids immunised, which is good, but they may
have put pressure on other services. (GS)
Secondly, Government stakeholders noted that vaccine objectors were often strongly
opposed to the requirements of the Measure:
The anti-vaxxers obviously hate this measure and are very vocal about it and trying to find
any loopholes or ways around it, which led to some challenges. (GS)
For those elements who aren’t in favour or are conscientious objectors, they have received
the policy in a negative way and if they’ve chosen not to meet the requirements their
payments are affected, and they have a negative experience. (GS)
The external stakeholders characterised recipients’ experiences with the implementation
more negatively than did government stakeholders. The external stakeholders generally
felt that recipients’ experiences were dependent on their child’s vaccination status,
highlighting the difficult experience many immigrants had in fulfilling their obligations, as
well as the perceived inadequate communication around the Measure from the
government. The external stakeholders felt that a lack of knowledge and confusion around
the implications of the Measure caused anxiety for many parents:
This caused a lot of angst, and a lot of angst for people who’ve come from overseas and
may not know the system. If their children are say 12–14 and have come 3–4 years ago,
they’ve suffered the most because they’ll often need catch-ups. English may not be their
first language. It can be quite traumatic, and they’re shoved from pil ar to post, they’re trying
their best and are being almost punished. They expect us to know things that we really just
didn’t know. (ES)
Social Policy Research Centre 2017
51
My sense is that the people who were impacted were either not wanting to get their kids
vaccinated or had lost track or never got around to it. But a lot of people probably did go to
get their kids vaccinated [as a result of the Measure]. We heard from the more difficult
cases I guess. (ES)
The policy has caused a tremendous amount of anxiety due to the threat of withdrawal of
payments, especially for parents who have thought they’ve done the right thing and want to
continue to do the right thing. For example, a father who moved from the Philippines and
was quoted $1000 to get his children’s immunisation record translated. He was desperate to
get his children registered and up to date. Eventually it was paid for him, but that was
incredibly complex and challenging. (ES)
Some external stakeholders also spoke of parents’ anger about the Measure with one
reporting that they had had to employ a security guard at their clinic to manage frustrated
and angry parents who were threatening staff:
Parents might’ve had to wait for the service because numbers went up and complexity of
cases went up, so we had people threatening harm to our staff, so we ended up employing
security guards at our clinics. We even had one person arrested because of the level of the
threatening behaviour they were exhibiting. I wouldn’t blame all this entirely on the policy
but it created that level of pressure on people to get caught up to avoid the potential impost.
(ES)
It is possible that parents’ anxieties and concerns could be related to the short time period
between the announcement of the Measure and its implementation. If some parents had
missed out on the announcement of the legislative change, notification of a potential
change in their family payments may have come as a shock, particularly if they were
unaware of how to rectify the situation.
4.5.1 Summary
Only the stakeholder component of the methodology provided any insights into the impact
of the Measure on the service delivery research question – has the service delivery model
resulted in impacted recipients having positive or negative encounters? An important
caveat is that these perspectives are a step removed from actual recipient experience of
the impact of the Measure. The government and external stakeholders’ views diverged,
with government stakeholders taking the view that recipients were largely receptive to the
Measure and had positive experiences overall. The key challenges they noted related to
updating immunisation records and opposition to the Measure from
conscientious/vaccination objectors. External stakeholders, on the other hand, appeared to
have more direct contact with affected parents and characterised their experiences more
negatively. They referred to perceived inadequate communication about the Measure, the
challenges faced by parents whose children were vaccinated overseas and parents’
confusion about the implications of the Measure. As noted by one of the external
stakeholders, it is likely that vaccination providers had more contact with parents who had
been negatively affected by the Measure than those who simply responded to the Measure
by updating their child’s immunisations without any complications. In addition, the vast
majority of recipients did not have to do anything – fill in any form, contact Centrelink,
ACIR or any vaccine provider, or change their behaviour – because their child(ren) already
met the vaccination requirements. It will be important to engage directly with parents in the
impact evaluation.
Social Policy Research Centre 2017
52
link to page 94 link to page 55 link to page 94
4.6 Communications
The PIR was guided by two key questions with respect to communications. These were:
• Did the communication strategy and Departmental communication plans
successfully support the implementation of the Measure?
• Did the Communication Working Group effectively manage communication issues
as they arose?
No documentation concerning the Communication Working Group (CWG) was provided to
the research team and subsequent communication indicated that the CWG was an
informal working group: it met on an ad hoc basis and no minutes were taken. The CWG
did not come up in the stakeholder consultations either. Therefore, the PIR focuses on the
first question above.
The Measure’s communication activities were a joint responsibility of DSS, Health, DHS,
and DET. The
Extending Immunisation Requirements (No Jab, No Pay) Communication
strategy, (Communication and Media Branch, 2015) from DSS finalised in November 2015
outlines the agreed overarching communication approach used by the Immunisation
Working Group. Complementary communication strategies were developed by DHS and
Health.
The
Extending Immunisation Requirements (No Jab, No Pay) Communication strategy
(EIRCS, hereafter) describes the aim of the strategy as ‘to raise awareness among target
audiences of the changes to immunisation requirements and the impact on CCB, CCR and
FTB Part A recipients’.
Table 3 below5, from the
EIRCS
(Communication and Media Branch, 2015, p. 5) outlines
the objectives of the strategy and the departments responsible for communicating with the
different audiences:
Table 3 NJNP communication objectives, department responsible & target audience
Objective
Responsibility
Audience
Inform
all families with
DSS, DET
Primary A
children under 20 (including
special audiences) about the
Families with children under 20 (including
proposed changes and the
families receiving these benefits and families
impact on payments
that might claim in the near future)
Raise awareness among
DHS, DSS, DET
Primary B
current CCB, CCR and FTB
Part A
recipients who do
Parents of children under 7 who do not meet
not meet the immunisation
the immunisation requirements and currently
requirements for their
receive CCB, CCR and/or FTB Part A
children of the steps to
supplement
catch-up on their child’s
5 Adapted to include the defined audience.
Social Policy Research Centre 2017
53
Objective
Responsibility
Audience
immunisations and ensure
Primary C
continuity of payments
Parents of children aged 7 to under 20 who
do not meet the immunisation requirements
and currently receive CCB, CCR and/or FTB
Part A supplement
Raise awareness of the
Health
Primary D
changes among
immunisation providers
Immunisation providers (including general
practitioners and immunisation clinics)
Details set out in Health’s
communication strategy
Inform
child care providers
DET
Secondary:
about the changes and
offering them information to
• Child care providers
pass on to their recipients (if
o Long Day Care providers
they choose)
o Family Day Care providers
o Outside School Hours Care providers
o Occasional Care providers
o In Home Care providers
• Child care peak bodies
• DHS service centre and call centre staff
including ACIR, Multicultural Service
Officers and Indigenous Service Officers.
• Family and Relationship Support
providers
The
EIRCS notes that the parents of incompletely immunised children fall into one of two
categories. These are:
1. vaccine objectors, and
2. ‘families who are behind in their immunisations because they face social, economic
or geographic barriers to access’ (p. 6).
The strategy notes that different communication strategies will be required for these two
groups.
The
EIRCS notes that vaccine objectors tend to be more affluent and educated and that
communication messages should focus on their right to vaccinate or not, but that choosing
not to vaccinate will result in losing eligibility for certain family assistance payments. The
EIRCS notes that the second category of parents whose children are incompletely
immunised is more likely to include larger families, single parent families and socially
isolated families. It notes that communication messages should focus on ‘the practical
support available to help their children catch-up on immunisations, including free vaccines
Social Policy Research Centre 2017
54
for current recipients’ (p. 6). The EIRCS notes that DHS would prepare a tailored
communication strategy for Indigenous and culturally and linguistically diverse families.
The communication strategy key messages are listed as:
• a five-point overarching narrative focusing on: the health of Australian children as a
Government priority; immunisation as the safest and most effective way to protect
against vaccine-preventable diseases; the real threat vaccine-preventable
diseases, like polio, tetanus and diphtheria, pose to our children; figures which
indicate that while Australia has childhood vaccination rates of more than 90 per
cent, a concerning number of children are not vaccinated because their parents are
vaccine objectors; and immunisation requirements for a number of family payments
as being strengthened in the interests of children’s health.
Additional key messages in the strategy relate to:
• changes to payments
• how to catch-up
• messages to child care providers; parents may become liable for the full cost of
child care, and providers can set their own policies about accepting unimmunised
children
• messages to health care providers; documented in the Health Communications
strategy.
The EIRCS lists a range of key issues that were foreshadowed as potential implementation
risks and the communication mitigation strategies that could minimise the risks. Identified
communication risks included:
•
complexity; the fact that the impact of the Measure varies depending on a range of
factors including the age of the child, and the type of payment received
•
segmented audiences; different audiences will require different information
•
timing; adequate notice needs to be given to affected families, however some of
the systems that support the new requirements would only be available from 1
January 2016
•
legislation; it was noted in the EIRCS, which was finalised in November 2015, that
the NJNP Bill would need to be passed by 3 December
•
drop dead dates; three different outcomes depending on the date the legislation
passed were outlined in the EIRCS
•
committee; the fact that the Bill was referred to the Community Affairs legislation
Committee for a public inquiry was noted as having a potential impact on the
implementation date
•
paid advertising; the costs and sensitive nature of the Measure were identified as
risks that would require review by the Special Minister of State
•
vaccine objectors; increased resistance from the anti-vaccination lobby was
identified as a potential risk, with the emphasis on choice to vaccinate or not as the
communication mitigation strategy of choice
Social Policy Research Centre 2017
55
link to page 62
•
child care service providers; concerns that child care centres may see an increased
in debts if families lose eligibility for payments
•
notifying lump sum recipients; the identified risk was that they would miss out on
the initial letter, but would be informed via indirect communication activities and
would receive letters later in 2016
•
cost of doctor appointments; vaccines would be free for eligible children but
families may still incur costs when they visit an immunisation provider
•
software used by immunisation providers; updates were required for the software
used to report children’s immunisation records, which could delay the reporting
process
•
impact on child care centres; a risk is that child care centres could be financially
affected by the Measure; therefore it would be important to communicate with child
care centres to ensure that they provide information to their families
•
Queensland, NSW & Victoria child care policies; the interplay between state-based
No Jab, No Play policies and the Australian Government No Jab No Pay Measure
would require tailored messages for the three states
In each case, the EIRCS outlines a communication mitigation strategy to minimise the
identified risk.
In addition to developing the EIRCS, DSS undertook a range of activities to support
implementation of the Measure. The minutes of the working group meetings outline the
actions taken by DSS and the other departments in the lead up to and after the
implementation of the Measure.
4.6.1 Department of Social Services
A budget of $277 377 (exc. GST) was allocated to the Department of Social Services
component of the communication activities (from DSS Response to questions on Notice 6
November 2016). A number of communication activities were undertaken by DSS to inform
parents, service providers and other stakeholders of the changes. Activities included:
•
information to child care centres; Child care centres would be sent information via
the Child Care Management System, which would include a printable PDF poster
that centres could display, immunisation-specific text to send to families in
newsletters, and questions and answers (See Section
4.6.4).
•
media pack: DSS prepared a media pack that included a joint media release, shell
announcements, talking points, questions and answers and newsletters.
•
social media campaign: The research team were provided with a final report (in the
form of a PowerPoint presentation) prepared by the media agency behind the
social media campaign initiated by DSS that aimed to raise awareness of the
changes associated with the introduction of the Measure (a final evaluation report
is under development). The Facebook campaign ran from 7 December 2015 to 18
March 2016, targeting particular audiences and regions, and delivered over 9.5
million impressions (advertisements) and a click-through rate of 0.48 per cent (the
Social Policy Research Centre 2017
56
link to page 94
12 February minutes report that the average government benchmark click-through
rate is 0.05 per cent). Advertisements linked with keyword searches delivered a
click-through rate of 2.66 per cent (linked keywords included: ‘no jab no play’,
immunisation, vaccination, immunise, ‘no jab’, vaccinate, ‘Centrelink payments’,
‘immunisation register’, ‘Family Tax Benefit’ and ‘immunisation schedule’. An
additional 7.25 million impressions were delivered. The campaign included
geographic targeting of low immunisation areas and high objection areas. These
often overlapped and included Coffs Harbour (NSW), Gold Coast (Queensland),
Epping (Victoria), and Perth (Western Australia).
It was noted in the 15 December minutes that the DHS
Immunising your children webpage
had a five-fold increase in visitors compared to the same time the previous year and that
the DHS ACIR webpage has also had an increase in traffic. The 7 December 2015
minutes noted that between 1 December 2015 and 8 February 2016 there were 541
mentions of No Jab, No Pay in the media on TV, radio and print news (including regional),
as well as online and on social media, and that only 12 per cent of the mentions were
negative. The 14 January 2016 minutes note that there were few media enquiries, with the
minutes attributing this to the media probably sourcing information from publically available
information on websites.
4.6.2 Department of Health
A communication plan from Health for general practitioners and vaccination providers was
developed as part of the 2015–16 Budget Measure commitment to funding complementary
measures to improve immunisation coverage rates
(Australian Government, 2015c). This
comprised $26.4 million over four years to Health to fund activities to:
• support parents and carers to make informed decisions about immunisation
• expand the National Human Papillomavirus (HPV) Vaccination Register
• provide a $6 incentive payment for vaccination providers who identify, call in and
vaccinate children up to seven years of age who are more than two months
overdue for vaccination, and record the information on the Australian Childhood
Immunisation Register (ACIR). Providers would receive a payment for each NIP
Schedule point caught up.
The communication plan lists:
• the communication objectives
• the target audiences for communication: primary audience includes general
practitioners and vaccination providers, with an emphasis on those working in rural,
remote and indigenous communities; and secondary audience is vaccine-hesitant
parents/guardians
• the stakeholders, including the Australian Indigenous Doctors’ Association, The
National Prescribing Service, Primary Health Networks, and state and territory
health departments
• the key messages for health professionals (about the new immunisation
requirements), changes to ACIR and messages for vaccine-hesitant parents and
carers (including reference to the development of new resources).
Social Policy Research Centre 2017
57
link to page 94
The communication plan notes the necessary collaboration with state and territory
governments and advisory committees for informing the content of the communication
products and activities developed. The communication plan outlines the resources that
would be developed, stakeholder engagement plans and information to be added to the
Immunise Australia website and hotline. The communication plan noted that Health would
communicate with vaccination providers prior to DHS undertaking the mail-out to parents
in November 2015
(Australian Government, 2015c).
The working group minutes report on the activities undertaken by Health:
•
catch-up information; the 8 December 2015 minutes note that catch-up information,
including factsheets, had been dispatched to vaccination providers in addition to
resources for vaccine-hesitant parents. The 18 December 2015 minutes noted that
there had been an increase in the number of children commencing immunisation
catch-up schedules. The minutes attribute this increase to confusion about the
grace period, with many people believing that they had to complete their
immunisations by 1 January or their payments would stop
•
the 18 December minutes also noted that there was confusion surrounding
conscientious objectors, with some people believing that if they enrolled by 31
December 2015 their conscientious objection would hold and they would receive
child care benefit for 2016. It was surmised that the source of this confusion may
have been information on the NSW Health site concerning the NSW conscientious
objection form. Further advice was provided to child care services to advise that the
NSW conscientious objection form related to enrolments and did not exempt
families from immunisation requirements for NJNP.
4.6.3 Department of Human Services
DHS also developed a communication implementation plan. The communication
implementation plan presented a ‘program summary’ that outlined the announcement of
the Measure and changes to immunisation requirements for eligibility for family payments
for recipients who receive:
• Child Care Benefit (CCB)
• Child Care Rebate (CCR)
• Family Tax Benefit Part A supplement
• Grandparent Child Care Benefit (GCCB)
• Special Child Care Benefit (SCCB)
• Jobs, Education and Training Child Care Fee Assistance (JETCCFA).
The summary noted that the immunisation requirement would apply to children and young
people up to age 20, that conscientious objection was no longer a valid exemption
category, and that the ACIR would be extended to capture immunisation details for people
up to age 20.
The communication implementation plan gives a summary of the four target audiences for
communication activities:
Social Policy Research Centre 2017
58
• parents and carers who receive CCB, CCR, FTB Part A, GCCB, SCCB or
JETCCFA
• vaccination providers
• third parties (community organisations, child care service providers, education and
training providers and software vendors)
• staff
The communication implementation plan notes that among the first group – parents and
carers – approximately 200 000 would be impacted by the changes and would need to
either ensure their child’s immunisation status was up to date, or seek a medical
exemption. The communication implementation plan emphasises that communication to
the second group – vaccination providers – should make it clear ‘that medical exemptions
should only be given for medical reasons indicated on the Immunisation Exemption
Medical Contraindication form’. The communication implementation plan noted that
although the third group – third parties – are not directly affected by the changes, ‘they
need to be informed about the changes so that they give correct information to customers
who will be affected’. The communication implementation plan noted that DSS was
responsible for communicating with this group. The fourth group was staff who ‘need to be
informed about the changes so that they give correct information to customers who will be
affected’.
The communication implementation plan outlines the objectives and key audiences for the
five key messages about the policy change and the potential impact on family payments if
a child’s immunisation status is not up to date. The document outlines the range of
communication activities targeting the four key audiences noted above. Activities targeting
recipients receiving the affected payments included updating webpages on
www.humanservices.gov.au, publishing articles in a range of outlets, publishing factsheets
in a range of languages, and posters. Activities including KPI metrics and costs are listed
in the communications implementation plan.
The communication implementation plan also notes the communication activities being
undertaken by DHS and Health targeting health professionals, parents and broader
community, members of the House of Representatives and senators, and media.
Communication with DHS staff has confirmed that the department is undertaking its own
post-implementation review to be completed in the near future.
In addition, the WG and IDC minutes outlined the range of communication activities
undertaken by DHS.
•
General information letters: The 15 December minutes report that DHS had
dispatched general information letters to 442 000 customers, receiving fewer
queries than anticipated.
•
CCB customers: The 15 December minutes reported that on 1 January 2016,
letters would be dispatched to 140 000 Child Care Benefit customers providing
formal advice that they will have entered the 63-day grace period. A second letter
would follow 30 days out from the end of the 63-day grace period.
Social Policy Research Centre 2017
59
•
FTB customers: The 15 December minutes reported that in March 2016, letters for
over 10 year old catch-ups to take to vaccination providers would be sent to FTB
customers and then to all cohort groups in May 2016.
•
Childcare providers: The 15 December minutes noted that childcare providers have
been included in a communication program with letters and posters dispatched on
15 December 2015 and that information on the DHS website was to be updated on
1 January 2016.
•
Information for CALD families: The 14 January 2016 minutes noted that DHS
Comms were working on translating short immunisation factsheets (366 words) into
22 languages to give culturally and linguistically diverse families background on
immunisation. These were to be published in PDF format.
•
Website update: In the 8 December minutes, DHS advised that 1 January 2016
was the earliest date possible to publish catch-up information on the DHS website.
•
Copies of the letters sent by DHS to families were provided to the research team:
These included a letter outlining the changes that were coming into effect and
advising parents/guardians to ensure their child was up to date with their
immunisations if they wished to continue accessing Family Tax Benefit6 and child
care fee assistance payments. The letter also advised how parents/guardians could
view their child’s immunisation history.
Additional letters were prepared for parents whose child(ren)’s immunisation status was
either:
• not assessed as up to date for their age
• unknown
• mismatched with information on file.
In each scenario, the letters clearly explained what actions the parent/guardian should take
to ensure that their family assistance payments were not impacted. The options for each
scenario varied, but included: logging on to the my.gov.au website to view their child/ren’s
immunisation history statement, calling the number provided and using the Express Plus
Medicare mobile app. Letters were also prepared for parents of children aged 10 years or
older whose access to child care fee assistance (Child Care Benefit and/or Child Care
Rebate) and Family Tax Benefit Part A supplement could be affected due to their child’s
incomplete immunisation status. Again, clear instruction was provided outlining what
actions parents should take, nevertheless, individuals with low literacy levels were likely to
struggle.
4.6.4 Department of Education and Training
The Child Care Payments Policy Branch was part of DSS before moving to the DET in
September 2015 through Machinery of Government changes. The Branch was responsible
Social Policy Research Centre 2017
60
for communicating with child care services (approximately 17 000) about the Measure. A
series of communication materials about the Measure was developed by DSS and
distributed via the Child Care Management System (CCMS) Helpdesk managed by DET.
These comprised of newsletters outlining the changes and posters for display in childcare
centres or for including in emails/newsletters to parents. Communications included:
• 14 December 2015; CCMS Newsletter Issue 79 outlining changes to immunisation
requirements from 1 January 2016 and a
No Jab No Pay A4 poster
• 18 December 2015, email; Clarification of NSW Conscientious Objection form not
being a valid exemption from NJNP changes
• 22 December 2015, email; Clarification of NSW Conscientious Objection form not
being a valid exemption from NJNP changes
• no date; Education Factsheet 20 –
No Jab No Pay: Changes to immunisation
requirements for CCB and CCR
• updated 1 July 2016; Factsheet 20 – What are the immunisation requirements for
Child Care Benefit (CCB)?.
4.6.5 Stakeholder perspectives
Most government stakeholders agreed that the Measure’s communications strategy,
including letters to recipients and health providers, as well as general media, was effective
in supporting implementation. At the same time, many were aware of issues that
hampered communications, including: the tight timeframe for implementation resulting in
delays in getting information to recipients and health professionals, the complexity of the
message7, and confusion due to different requirements for different payments.
Positives of the communications strategy included consistency in delivering the same
message across departments and utilising as many channels as possible to communicate
the changes resulting in high levels of awareness.
Everyone worked very closely together across departments to make sure we were all
delivering the same message, and using as many channels as possible and getting as
many individuals as possible, across health professional to parents and guardians. (GS)
It got a lot of reach, and it was really strongly reported in the community and there was a
high level of awareness with our customers and the community at large. ‘No Jab No Pay’
term as a term has gained a lot of currency and has resonated in the media and the
community. There’s no doubting the effectiveness of the awareness of the policy in the
community. (GS)
Communication delays due to the short timeframe between passing the legislation and
implementation caused confusion for some parents who needed to update their child’s
immunisation records. Additionally, immunisation providers who were directly impacted by
the Measure were identified as being inadequately prepared and supported.
7 Communication from DSS indicates that all letters were reviewed by multiple stakeholders, including the
relevant policy departments, to ensure that the language was clear and understandable.
Social Policy Research Centre 2017
61
A letter could’ve gone out earlier than it did to tel parents what to do if their child was
incorrectly noted as not on the register. But this should’ve been anticipated as it was a
known issue beforehand. (GS)
We wrote to every GP and provider in the country pre January 1. It was fairly effective.
Some said they hadn’t received enough notice. There was an influx into GPs of people
needing to sort out complicated catch-ups and so on, so the feedback from health providers
was that that was onerous and that no support was given for that. (GS)
Two government stakeholders had different perspectives on communications to recipients.
One felt that the message was clear and that recipients had misinterpreted the letters,
while the other felt that the complexity of the message caused confusion for recipients:
For parents, there was some misinterpretation of letters sent to them. There might’ve been
a lot of frustration from those who may have been up to date but got a letter saying they
weren’t up to date. This was actually just Centrelink saying “We haven’t established a link
between ACIR and Centrelink” and didn’t know if they were up to date rather than saying
they weren’t up to date, so people panicked, but they’d ask the doctor who would say “No,
you are up to date”. So the letters were clear on how this all worked, but people tend to not
to read them properly. (GS)
Our only option for directly speaking to customers was through the DHS letters. The letters
themselves are complex, so our communications tried to support the context and strategy of
the change and give a call to action. It was a combination of a complex message to get
across, and perhaps flaws in the messaging itself. There were clear calls to action to do
something from the DHS letters. (GS)
This same stakeholder who felt that recipients may have misinterpreted government
communications also felt that health providers may have run into trouble because they too
had misinterpreted the requirements of the Measure that had been communicated to them:
For health providers, some of them just don’t understand vaccination catch-up schedules
and when children need certain doses. They need better education. Sometimes they have
trouble interpreting the Australian Immunisation Handbook, which is what they’re supposed
to go by. (GS)
One government stakeholder acknowledged that the new requirements were not entirely
clear for FTB recipients, noted that a media release gave the impression that the Measure
affected FTB payments, not just the supplement.
The external stakeholders were generally less positive about communications surrounding
the Measure. Most explained that they had not received adequate information about the
Measure, or that there were gaps in the information provided to them by government. This,
in turn, hindered their ability to explain the changes to recipients:
DHS and DSS8 sent letters to the parents about being cut off and we never saw those
letters – we just get a flurry of parents ringing us and that’s the first thing we know about it.
(ES)
Some GPs even rang us about the letters because they just said ‘you’re overdue’, but they,
and we, didn’t know what they were overdue for. So yeah, I don’t know what the
communications plan was but they sure didn’t show us. We weren’t part of the plan. (ES)
8 This is factually incorrect as no letters were sent by DSS.
Social Policy Research Centre 2017
62
There wasn’t enough information. The main information we received was from the Chief
Public Health Officer and other info that trickled through the state jurisdictions. Not sure if
they were receiving adequate info but at our level we weren’t. (ES)
Additionally, some external stakeholders said that the quality of information provided to
parents was of poor quality, especially for recipients with low literacy levels:
The letters were very confusing – they had a lot of words but didn’t say anything. We know
that literacy is an issue for a lot of people. (ES)
It didn’t work. They had four different letters to parents depending on their particular
circumstances. They were so lengthy and so confusing, for people where English wasn’t
their first language or they had learning difficulties, the communication was extremely poor.
I did hear that parents had said that they had been onto Centrelink and tried to get
information from them and would have to wait in excess of 90 minutes on hold. (ES)
4.6.6 Summary
Communication strategies developed by DSS, DHS and DET supported implementation by
outlining the key messages about how the Measure would affect eligibility or child care and
family payments. Although not strictly part of the Measure, a communication plan from
Health outlined communication activities with general practitioners, vaccination providers,
and key stakeholders in state and territory health departments.
Most government stakeholders felt the Measure’s communications strategy was effective in
supporting implementation. However, they identified a number of issues that hampered
communications including: the tight timeframe for implementation resulting in delays in
getting information to recipients and health professionals, the complexity of the message
and confusion due to different requirements for different payments. On the other hand, the
government stakeholders also identified a number of positives of the communication
strategy. These included consistency in delivering the same message across departments
and utilising as many channels as possible to communicate changes, resulting in high
levels of awareness. External stakeholders were generally less positive about
communications. They felt that the information provided to them and to recipients was
inadequate, which hindered their ability to explain the changes to parents/guardians.
4.7 Management information
The PIR also looked at how the policy and system design impacted upon the data
available to date regarding rates of immunisation and eligibility for family assistance (both
Family Tax Benefit Part A supplement and child care payments).
The document review highlighted concerns about the quality of the data in the ACIR,
ongoing capacity to monitor conscientious objectors in the future, issues concerning data
linkages between the Centrelink system and the ACIR, and the management information
that was produced to monitor the implementation and impact of the Measure. Findings
from the stakeholder consultation primarily concerned the issues of updating the ACIR and
the data quality.
Social Policy Research Centre 2017
63
4.7.1 Australian Childhood Immunisation Register (ACIR)
Prior to the implementation of the Measure, several submissions to the Senate Community
Affairs Legislation Committee inquiry highlighted concerns about the data quality in the
ACIR. These included concerns about:
• the accuracy of the data in the ACIR;
o Professor Leask’s research suggested that possibly between 18 to 50 per
cent of records might incorrectly show that children were not up to date with
immunisation (Senate Community Affairs Legislation Committee, 2015: 24;
Leask 2015, submission to inquiry)
o a submission from NSW Health noted that inaccurate data may be due to
data transfer issues and that the vaccination status of children over 7 years
was not previously available in the ACIR
• an inability to monitor conscientious objection if the Bill was passed.
Data quality
In the light of the concerns about data quality, in the Senate inquiry the Greens proposed
delaying the implementation of the Measure until July 2018 so that concerns could be
addressed. It is noted in the minutes from the 23 November 2015 meeting of the
Interdepartmental Committee (IDC) that delaying implementation until 2018 was not
possible because ‘the supplements are due to be phased out by this date’. The Committee
also reported that both Health and DHS were taking action to improve data quality.
Stakeholders noted that implementing the Measure necessitated a significant amount of
additional information being entered into the ACIR, particularly for those children from 10
to 20 years of age who had previously not been included. Linkages between the Centrelink
payment database and the ACIR also needed to be updated with the influx of new
information and requirements of the Measure.
Several government and external stakeholders commented that the data quality within the
ACIR had improved, but that it had come at the cost of short-term issues, including delays
uploading data, data cleaning and parental angst:
It’s created a lot of manual intervention being required that was never required before, for
example cleaning up duplicate data or rubbish data or incorrect reporting of dose numbers.
And because ages have extended up to 20 [years old] there’s a lot more work involved.
(GS)
The ACIR was absolutely overwhelmed … for months a lot of records were pending, which
means the child isn’t considered up to date. There was a lot of manual intervention required,
which is a huge demand for this scale of program. There was no real opportunity to work
through those issues before the Measure was implemented. (GS)
So a lot of the data was incorrect in the first place due to human error and software errors.
So [the Measure] was a success in that it identified where the data was incorrect and
needed fixing, but that shouldn’t have been at the expense of parents’ anguish. (GS)
Other government stakeholders referred to the additional work to establish linkages
between DHS and the ACIR that were required for the Measure. It was acknowledged that
Social Policy Research Centre 2017
64
the process was not without its challenges but that the linkages were ultimately
successfully established:
There has been ongoing work with Centrelink to establish those checks and balances,
which were successful in the end, but not real y ‘smooth’. We’re constantly working and
looking to see if there are any issues with the data. (GS)
To expand the ACIR, which was a requirement of the policy, we then therefore had to re-
examine the way that we linked records and ensure that we had as robust a process as we
could develop, within the limitations of the system that we have to conduct those linkings.
(GS)
Two government stakeholders theorised as to why there were so many issues with the
ACIR and why there may have been so much missing immunisation data. The first
suggested that perhaps many doctors had simply not uploaded children’s immunisation
histories to the ACIR. Alternative explanations included operator errors at DHS or issues
with the ACIR. The second stakeholder suggested that many immunisation providers might
not be adequately skilled at entering the data into the register. This stakeholder recalled
how, in the past, there were ACIR liaison officers in every state and territory who would
liaise with immunisation providers about uploading information to the ACIR:
[Their] remit was to help with data quality and cleaning, and educate providers on how to
use the system. Their role was ceased about 3 or 4 years ago. They were very useful to
field questions, look at problems. (GS)
One external stakeholder argued that the ACIR should have been subject to a complete
overhaul prior to the implementation of the Measure rather than having efforts made to
simply update it, as successful as these efforts may have been in the short-term:
I think the policy has driven attempts to improve the data and the register. At its heart the
register is very poor. It was built in the 1990s. It takes me five minutes to log in. It’s an
ancient piece of infrastructure that should have had a complete revamp before undertaking
a measure like this. (ES)
Conscientious objectors
A number of submissions to the Senate Inquiry expressed concern that conscientious
objection would no longer be recorded in the ACIR. Submissions recommended either the
retention of objection provisions in the data set or that the government should attempt to
survey the rate of conscientious objection annually (Leask submission).
4.7.2 Implementation
Data linkage – ACIR/AIR & ISIS (managed by DHS)
With receipt of child care and family payments being conditional upon up to date
immunisation status, data linkages between a child’s ACIR/AIR records and the Centrelink
program’s Income Security Integrated System (ISIS) records are critical. The Extending
Immunisation Requirements Detailed Requirements Document (EIR DRD) outlines the
changes made to ACIR/ISIS system to facilitate data exchange, enable assessment of
entitlements, orchestrate mail-outs, enable recipients to provide information, and provide
assistance to staff. DHS EIR staff training documents note that data linkage is established
Social Policy Research Centre 2017
65
via the child’s Medicare number and offer advice on how a link can be established if the
child does not meet the residence requirements for Medicare.
Vaccination objection
The term ‘vaccination objection’ was used to replace ‘conscientious objection’ in the ISIS
data. Before March 2013, vaccination objections were recorded at Centrelink on the ISIS
mainframe (EDW), the ACIR or on both. The EIR DRD 15.7 notes that up to 100 000
conscientious objections were recorded on the ACIR for children up to 20 years of age.
This historical vaccination objection status still exists in the EDW data.
Monitoring implementation
The EIR DRD documents the management information data requests by Departments for
the purpose of monitoring the implementation and impact of the Measure. These include a
wide range of data requests from ACIR and DHS data system, including ACIR data on:
• the number of vaccination objections recorded on the ACIR system
• the number of children for whom an objection is registered but then the child met
full vaccination status
• the number of legacy vaccination exemptions (at 31 December 2015).
Regular reports from Centrelink (DHS) data were to be provided to, DSS, DET and Health,
and relevant Ministers including:
• a count of Immunised Children (total)
• the number of children with immunisation exemptions
• the number of immunisation overrides
• the number of children who are not linked to ACIR
• the Immunisation Status (child)
• the Immunisation Status Reason (child) (e.g. override, exemption, fully immunised,
etc.)
• the Immunisation Link Status (child)
• the Immunisation Link Reason (child)
• the Immunisation Requirement – (milestone at which child is currently active
• a CCB/CCR Indicator – whether a recipient is current CCB Only, CCB/CCR, CCR
Only or claim pending
• FTB-A Immunisation Supplement Withheld – Child.
A range of reports (short-term, interim, one-off, and ongoing) were required for the child
care and family payments that were linked to immunisation status with the introduction of
the Measure. The purpose of the reporting was to determine whether the Measure had
resulted in any changes to the number of families receiving payments.
Additional reports that were described in the EIR DRD included a report on the
effectiveness of the data integrity exercise each time it was conducted, and a report on a
quarterly basis for the National Centre for Immunisation Research and Surveillance
(NCIRS) that includes all children on the register and their associated valid vaccines.
Social Policy Research Centre 2017
66
4.7.3 Summary
The introduction of the Measure has led to significant changes in the data collected
through ACIR/AIR on rates of immunisation. The review of documents and stakeholder
consultation suggests that there were many challenges in this process, some of which
were due to the short lead time to implement the Measure once legislation was passed.
The stakeholder perspectives suggest that the changes were eventually successfully
implemented, which may result in higher quality data on rates of immunisation for
Australian children and the extension of this data to children up to age of 20 years. One of
the tasks of the impact evaluation should be to examine the quality of the data on
immunisation rates in the ACIR/AIR. While the DHS data contains historical information
recorded on registered vaccine objections, the capacity to monitor ongoing levels of
vaccine objection in the national community has been reduced. Options to continue to
monitor conscientious objection, as part of a broader inquiry into community understanding
and confidence in vaccines, should be examined as suggested by submissions to the
Senate Inquiry.
Social Policy Research Centre 2017
67
5 Discussion
The Post Implementation Review (PIR) of the No Jab, No Pay
2015–16 Budget Measure
was undertaken to assess implementation successes and challenges, and also to inform
the development of the impact evaluation Framework. This framework is presented in the
following section.
Overall the implementation of the Measure went relatively smoothly from a policy
perspective. Governance arrangements, risk mitigation strategies and communication
strategies were put into place, and the Measure was implemented in a flexible manner that
allowed for challenges to be addressed as they arose. Government departments worked
well together and the communication between departments was effective in addressing
overlaps and gaps. There were additional benefits to the implementation of the Measure,
in particular improvements in the accuracy and completeness of the AIR.
A key implementation challenge identified by all stakeholders related to the short
timeframe for implementing the Measure. With the announcement of the policy in April
2015, the passing of the legislation in November and implementation on 1 January 2016,
those responsible for implementing the Measure and communicating the changes to
affected parents faced significant challenges. Yet, despite the tight timeframe, it appears
that implementation went relatively smoothly from the policy implementation side. Two key
implementation challenges related to the need to extend the payments beyond the initial
grace period for existing recipients due to delays in uploading immunisation data to the
AIR. A second challenge was the need to amend the continuous/rolling catch-up anomaly
to ensure that parents who were not committed to immunising their child were not placed
on a six-month catch-up repeatedly. A key system success relates to system
responsiveness when issues were identified, with both of these issues being addressed
promptly, thereby limiting negative impacts for recipients.
Despite the effective implementation by the Australian Government, there were
considerable difficulties for state and territory officials as well as vaccination providers.
Several external stakeholders felt that the policy was designed without consideration of the
impact the Measure would have on the workloads of general practitioners, immunisation
providers and other allied health professionals at the state level. These challenges were
compounded by:
• the short timescales for implementation
• the lack of additional resources provided for states and vaccine providers, other
than the $6 incentive
• inaccuracies in the ACIR and backlogs in getting data uploaded onto the database.
Implementation of the Measure also required effective communication strategies to ensure
that families were made aware of the changes. Many external stakeholders felt that
communication about the Measure was poor and confusing for affected families, referring
to parents’ anxiety, frustration and confusion when advised that their child’s immunisation
records were not up to date.
Social Policy Research Centre 2017
68
link to page 96 link to page 94 link to page 96
Communications about the Measure provided mixed messages about the focus of the
Measure on parents who objected to vaccination. The DSS communication strategy
(EIRCS) noted that the parents of children not fully immunised were either vaccine
objectors, or ‘families who are behind in their immunisations because they face social,
economic or geographic barriers to access’ (p. 6). The strategy noted that different
communication strategies were required for each category of parent. One of the key
messages to vaccine objectors was that they had a right to vaccinate or not, but that if they
chose not to, they would lose eligibility for certain family assistance payments.
At the same time, the EIRCS outlined a five-point overarching narrative focusing on: the
health of Australian children as a government priority, immunisation as the safest and most
effective way to protect against vaccine-preventable diseases and the ‘concerning number
of children [who] are not vaccinated because their parents are vaccine objectors’ (p. 8).
Despite the fact that available data suggested that vaccination objectors constituted under
a quarter of the incompletely immunised, media around the Measure tended to focus on
this group of parents. This focus on vaccination objectors created the impression that they
were the target of the policy, with a number of stakeholders questioning whether this focus
was misguided. This impression is confirmed by the extract below from a 2UE interview
with Minister Porter in November 2015 when the Bill was passed:
What we did was we took the best available scientific advice and evidence. Scientists talk
about a level of herd immunity which is that point that you require to effectively control the
transmission of an infection amongst a population and that varies from disease to disease,
but those diseases that I’ve just mentioned, that herd immunity level is 95 per cent, and we
in Australia were dropping below that level of group immunity because of the very large
number of what were known as conscientious objectors. And we felt, as a government, that
we needed to rectify that situation.
(Porter, 2015)
Despite this statement of the primary purpose of the Measure, DSS reported to the Senate
inquiry that it did not expect that the Measure would significantly alter rates of
immunisation among conscientious objector families. DSS’ assumptions were that the rate
of children with a recorded vaccine objection in the FTB Part A population would drop from
just 1.8 to 1.5 per cent as a result of the Measure. DSS reported that it expected that the
majority of families who immunised their children as a result of the Measure were expected
to do so as a result of eligibility being checked each year until age 20. Thus, one aspect of
the modelling undertaken by the Department on the reduction of VOs was more
conservative than the policy intention.
As noted above, the intended goal of the policy was not to provide budget savings, but to
protect public health by increasing immunisation rates
(Abbott, 2015). Although budget
savings was not the goal of the policy, failure to meet immunisation requirements was
expected to result in significant cost-savings for government. DSS figures provided in
response to a Senate Inquiry question on notice showed that 563 500 children were
expected to fail the immunisation requirement over 4 years (2015/16 to 2018/19). The
majority of these children (65–70 per cent) were aged 10 years or over. DSS expected that
in 2016/17 around 10 000 families would lose an average of $7 000 in child care payments
and that 75 000 families would lose the FTB Part A supplement, which is currently $726.35
(Report of Senate Community Affairs Legislation Committee, 2015, p. 8).
Social Policy Research Centre 2017
69
An issue not identified in the document review or by stakeholders was whether some
recipients facing practical and logistical barriers to updating their immunisations (rather
than vaccine objection) would lose payments as a result the Measure. This issue should
be explored in the impact evaluation.
Overall, the majority of the challenges identified by the PIR can be accounted for as
‘teething problems’ which are to some extent inevitable in the implementation of any
complex measure, particularly when this is required in a short time frame with little
opportunity for preparation. It is anticipated that most of these challenges will be resolved
and will not affect implementation in the long-term. Perhaps the only long-term unintended
consequence of the Measure has been the loss of ability to track conscientious objectors,
and henceforth the government will need to rely on proxy measures to assess the extent of
conscientious objection in the community.
One of the biggest challenges for this Measure relates to the messaging around its
implementation. Three broad messages were provided in communications around No Jab,
No Pay:
• a change to the behaviour of conscientious objectors
• encouragement to those who are hesitant or face logistical problems to fully
vaccinate their children
• a cost-saving measure.
It is inevitable that complex policy initiatives will have multiple objectives, and of course
government is not in control of how the media reports policy developments. Nevertheless,
these inconsistencies in the messaging around this Measure have resulted in much
cynicism amongst some key stakeholders and have not been helpful in the early
implementation. These three messages are all based on sanctions and self-interest rather
than providing positive messages to the population about the need for vaccination, the fact
that it is safe for the vast majority of children, and the contribution families can make by
ensuring that their children are fully vaccinated.
Although the early implementation has been mostly successfully accomplished, it is not yet
possible to assess whether the Measure itself has been successful. There are early
indications that vaccination rates have improved, but this could be accounted for in a
number of different ways, including improvements in data collection and recording. The
evaluation will need to assess the degree to which the Measure has not only improved
administrative processes, but has led to actual changes in population behaviour, and
whether these have been sustained over time.
Social Policy Research Centre 2017
70
6 Impact Evaluation Framework
Drawing on insights gained through conducting the PIR, this section of the report presents
a range of options and strategies for the impact evaluation of the No Jab, No Pay 2015
Budget Measure. Before outlining the proposed impact evaluation framework, we present
the No Jab, No Pay
Theory of Change and policy logic model.
6.1 No Jab, No Pay theory of change
The broad purpose of a ‘theory of change’ is to articulate and map how a program,
intervention or policy is expected to lead to change or, in policy terms, to achieve the
desired policy outcome. In addition to including the program or policy that is expected to
produce change, the theory of change also looks at other environmental and contextual
factors that might contribute to the desired change.
The aim of the Measure is to increase immunisation rates by linking eligibility for child care
and family payments to immunisation status. However, a range of additional factors could
also lead to higher rates of immunisation. This makes the impact of the Measure on
increasing immunisation rates difficult to separate from the contributory impact of other
factors. In addition the Measure itself contains a number of components, and was
accompanied by associated measures (e.g. incentive payments to vaccination providers)
as part of a package of reforms. The evaluation will, as far as possible, identify the
effectiveness of different components of the Measure and its associated changes.
The Measure strengthened the immunisation requirements that apply to Australian
Government child care payments and the FTB Part A supplement. The three policy
mechanisms utilised were: the removal of conscientious objection (now called vaccination
objection) as a valid exemption category, the extension of eligibility monitoring up to 20
years, and the removal of the initial grace period for new recipients to get up to date with
immunisations.
The main component of the theory of change asserts that the prospect of losing eligibility
for child care and family payments would prompt parents to ensure that their children’s
immunisations were up to date. The desired outcomes were:
• that parents of children who were assessed as not fully immunised might get their
immunisations up to date
• that parents who had a registered ‘conscientious objection’ to vaccination might get
their children immunised.
If these outcomes are achieved, the immunisation rate will increase. If these outcomes are
not achieved, the parents of children assessed as not fully immunised will lose eligibility for
payments, resulting in savings for government.
In addition to the Measure, Figure 1 No Jab, No Pay theory of change below identifies a
range of additional factors that might also have an impact on increasing immunisation
rates. These include:
Social Policy Research Centre 2017
71
• the general practitioner/vaccination provider incentive payment scheme (it has not
been possible to access any data from Health concerning uptake of the scheme)
• more accurate and timely recording of immunisation data in the ACIR
• health-funded activities to improve the community’s understanding and awareness
of the National Immunisation Program (NIP)
• improved vaccination reminder systems (e.g. The Victorian Department of Health’s
VaxOnTime app)
• state-based
No Jab No Play policies
• a communications campaign
• media coverage of the Measure.
Social Policy Research Centre 2017
72
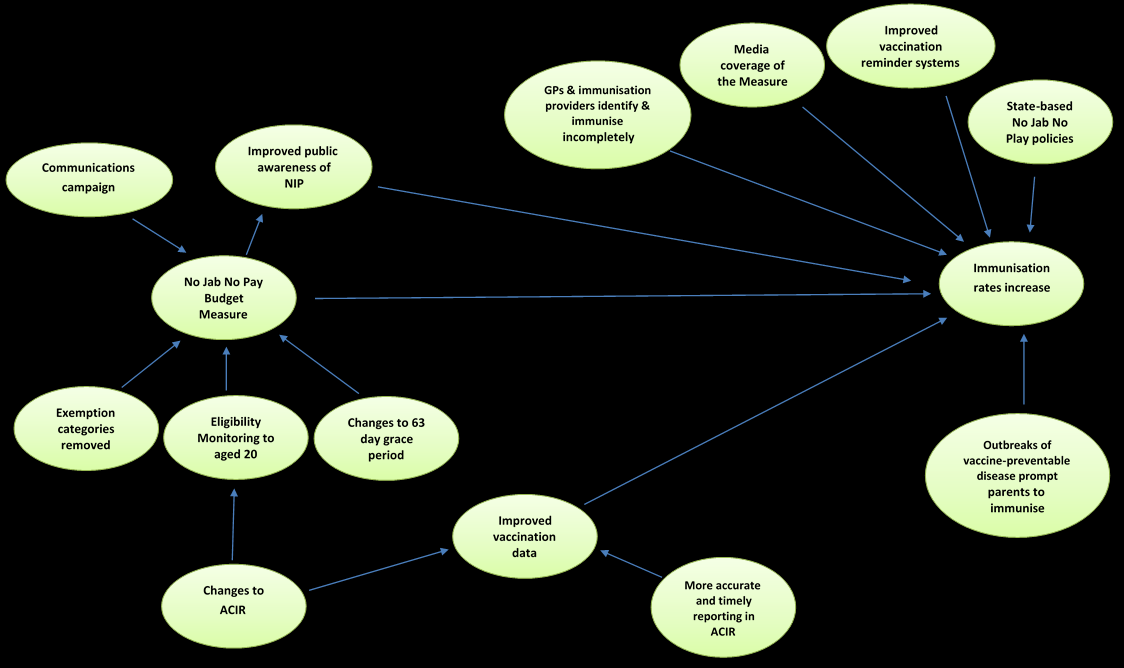 Figure 1 No Jab No Pay Theory of change
Figure 1 No Jab No Pay Theory of change
Social Policy Research Centre 2017
73
link to page 78
6.2
No Jab No Pay Policy logic
Articulating the No Jab, No Pay (NJNP) policy logic requires consideration of policy
design (‘sticks’ and ‘carrots’), how the policy will be implemented (system, data,
governance, communications etc.) and the intended impact.
The logic of the NJNP policy design involves strengthening conditionality through
three mechanisms:
• eliminating exemptions for conscientious/vaccination objection
• making changes to eligibility monitoring (up to 20 years)
• removing the initial grace period for new recipients.
Although not part of the Measure, a range of complementary measures were also
undertaken by Health, including: incentivising general practitioners and vaccination
providers to identify and immunise children (under 7 years of age) who were more
than two months overdue for their vaccinations, improving public vaccination records
and reminder systems, and making efforts to increase public awareness of the
benefits of vaccinations.
Implementation required a range of inputs, including funding, governance structures,
communications and data management systems. The ultimate aim of the Measure
was to increase immunisation rates and sustain them at herd immunity level (95 per
cent or better). The NJNP policy logic model below
(Figure 2) outlines the inputs,
activities, outputs, outcomes and impacts of the Measure
. It is important to note that
the impact evaluation will aim to establish the effect of the Measure on the outcomes
listed in Figure 2, but is unlikely to be able to do so with respect to the listed
impacts.
6.2.1 Unintended consequences
While policies may be designed to target specific populations, there is always the
potential for unintended consequences. Concerns were raised in the Senate Inquiry
about the potential impact of the Measure on children of parents who may face
barriers to immunisation, or whose records are incomplete for a range of reasons.
The impact of the Measure and loss of eligibility for child care payments and FTB-A
supplement could result in:
• increased inequality in incomes if families with lower levels of incomes are
those facing practical and logistical barriers and do not commence catch-up
schedules
• consequences for family and child wellbeing due to either:
o not being up to date with immunisation; or
o records being inaccurate
• parents withdrawing their children from child care, with resulting education
and social disadvantages
Social Policy Research Centre 2017
74
• parents withdrawing from the labour force due to lack of childcare options,
resulting in reduced family income
• less vaccination provider engagement/communication with vaccination
objectors
• longer term impact on public confidence in public health because of negative
messaging rather than the promotion of the positive contribution made by
vaccination
• increase in rates of medical exemptions as a result of the category of
conscientious objection no longer being available.
A key objective of any impact evaluation would be to examine the extent to which
the introduction of the Measure has had unintended impacts on different sectors of
the population.
Social Policy Research Centre 2017
75
Figure 2: No Jab, No Pay Policy logic model
Inputs
Activities
Outputs
Outcomes
Impacts
Funding/resourcing:
• Strategies to enable
• Development of
• Increased immunisation rates
• Reduced incidence
implementation of Measure
parent/vaccination
(N.B. baseline issues due to
of disease
• DSS
& interdepartmental
provider/childcare
imperfect ACIR data)
• Healthier children
• Health
collaboration are
provider information
• Increase in incompletely
• DHS
adequately funded
resources
immunised children engaging
•
•
DET
Expansion of ACIR
in catch-up schedule
•
•
Incentive payments for
Decline in vaccine objectors
vaccination providers
• Records of recently arrived
(Health
children updated in ACIR
complementary
• Savings or revenue neutral?
measure)
• Improved VP/parent
• Health providers
communication/engagement
(general practitioners
leading to greater willingness
& immun. providers) –
to immunise
follow up & immunise
children who are not
fully immunised
Project plan (DSS)
• Detailed implementation
• Vaccination providers
Improved monitoring of
plan developed
updating AIR in timely manner population health
• Stakeholders engaged &
Availability of sufficient
• Greater knowledge among
consulted
vaccines assured
vaccination providers about
immunisations
• Greater understanding among
Childcare providers inform
childcare providers about
parents about potential
vaccination requirements
policy impact
76
Inputs
Activities
Outputs
Outcomes
Impacts
Communication
Communication strategies
• Letters to parents
• Greater awareness among
• Improved vaccine
strategy
developed:
• Info to immunisation
public & immunisation
confidence among
providers
providers about policy change
parents
•
•
with respect to improved
DSS
• Overall & within each Dept.
Info to childcare
•
health (incentive payment for
DHS
• Communications working
providers
•
•
vaccination providers –
Health
group meetings/actions
Media activity
•
Health) and ‘strengthening
DET
• Between the Australian
eligibility requirements’ for
Government & states
•
family payments (DHS)
Between states and
vaccination providers
Governance
• DSS lead agency
• Reports
• Clear delineation of
• Long-term
• Working group and
• Minutes
responsibility
sustainability of
Interdepartmental
• Actions
• Greater collaboration between
Measure
Committees established
stakeholders
• Internal communication
• Improved ability to pre-empt
pathways articulated
issues & risks
• Risks & issues documented
• Decision-making
mechanisms established
Data linkage/
•
DHS – EDW, ISIS
•
Data records/reports
•
Accurate, timely lifetime data
• Improved public
management strategy
•
Health – ACIR
health monitoring
•
DET – Child Care
Management System
•
Software – immunisation
providers
•
Management information
Social Policy Research Centre 2017
77
6.3 Data Scoping
The data scoping component aimed to develop options on how departmental
datasets might be utilised in the impact evaluation. The objective of the data
analysis in the impact evaluation would be to review changes in immunisation rates
for the target populations and also to examine whether there have been any
unintended consequences. With regard to the associated measures, the impact
evaluation should also assess data, if available, on:
• the role and take-up of Health incentive payments
• performance benchmarks for states and territories
• the impact of the community awareness campaign.
6.3.1 Changes in immunisation rates for target populations
As outlined above in this report, the target populations of the Measure are parents
and carers of children who are not fully immunised. This group comprises children
with parents with registered and unregistered vaccine objections and those who are
not fully immunised for other practical and logistical reasons that may relate to
socio-economic or other disadvantages.
Data for the impact evaluation would aim to analyse the change in immunisation
rates for the following population targets:
• children who currently have a registered vaccination objection by
o income levels of parents
o socio-economic status of area (SA3)
o vaccination status (partial, none)
• children not up to date/meeting immunisation requirements and with no
registered vaccination objection, including those:
o whose immunisations are up to date but there are recording errors in
ACIR
o whose parents are silent unregistered objectors
o whose parents have not immunised their children due to practical and
logistical reasons:
▪ with disability
▪ from low income families
▪ in lone parent families
▪ large families (3 or more children)
▪ from low SES areas
▪ from more remote areas
▪ are temporary migrants
▪ born overseas
Social Policy Research Centre 2015
78
• older children who had not previously been immunised (aged 7–20 years) to
identify changes in immunisation rates of the older child population.
As well as looking at changes in immunisation rates between two points in time (or
pre and post the implementation of the Measure), the analysis would also aim to
track the trajectory in the rates of change, that is, whether there is an initial increase
in immunisation rates, which is sustained over a medium and longer period.
6.3.2 Assessing the impact of unintended consequences
As noted above, the document review and stakeholder consultation highlighted
specific groups of children that should be a focus of this analysis of potential
unintended consequences. The analysis could therefore use Departmental data
associated with the Measure to map loss of payments and subsequent changes in
family incomes, childcare attendance, and parental employment status for families
with children:
• with disability
• from low income families
• in lone parent families
• in large families (3 or more children)
• from low SES areas
• from more remote areas
• of temporary migrants
• of refugees or asylum seekers
• born overseas
• from Aboriginal and Torres Strait Islander communities;
• who hold a health care card
• whose parents hold a health care card, pensioner concession card, or a
Veteran’s Affairs Gold or White card
• that are known to child protection, are living in emergency or crisis
accommodation, or are of no fixed address due to family violence or
homelessness.
Departmental data could be used to assess any increase in rates of medical
exemptions that may be attributable to the category of conscientious objection no
longer being available.
In addition, the impact evaluation analysis could explore other data sources, or
develop a dedicated survey to assess the impact of the Measure on:
• vaccine provider engagement/communication with vaccination objectors
• public confidence in vaccines.
Details of departmental data and potential options for analysis are outlined below.
Social Policy Research Centre 2017
79
link to page 83
6.3.3 Data sources and data analysis options
On the advice of the Department of Social Services the following data sources were
reviewed and information sought from the data custodians as to data items, data
quality, and processes for data access. The data sources are outlined i
n Table 4.
Australian Childhood Immunisation Register (ACIR)/Australian
Immunisation Register (AIR)
The ACIR became the AIR on 30 September 2016. The ACIR/AIR data custodian is
Health. The current population in this database includes all children aged 0–20
years with a Medicare record, and all children who have had immunisation records
uploaded by immunisation providers.
The ACIR/AIR data also includes information on types of exemptions for
immunisations, including data on registered conscientious objectors. Data on the
number of children with a conscientious objection registered between 1999 and
2015 is publically available.
A wide range of publically available reports exist on data from the ACIR including:
• annual historical data on immunisation rates for states and Australia for 3
cohorts (12–<15 months, 24–<27 months, 60–<63 months) from 1999–2015
and current data for these cohorts based on year to June 2016
• annual historical data for Aboriginal and Torres Strait Islander children on
immunisation rates for states and Australia for 3 cohorts (12–<15 months,
24–<27 months, 60–<63 months) from (2003–2015) and current data based
on year to June 2016
• quarterly immunisation data for SA3s (from March 2015 to June 2016)
• Primary Health Network Immunisation Coverage Reports
• Annual National vaccine objection (conscientious objection) data from 1999–
2015
• quarterly state and territory data vaccine objection (conscientious objection)
data from 2012–2015
• National Health Priority Areas reports on national immunisation rates 2012–
13 and 2014–15
• National Centre for Immunisation Research & Surveillance (NCIRS) reports
on Annual immunisation coverage reports, Australia (2007–2014)
• NCIRS reports on Annual immunisation coverage reports, Australia (2009–
2015)
• Public Health Information Development Unit (PHIDU) – Social Health Atlas –
children fully immunised at 1, 2 and 5 years (2015)
• PHIDU – Social Health Atlas – Aboriginal and Torres Strait Islander children
fully immunised at 1, 2 and 5 years (2015)
Social Policy Research Centre 2017
80
Table 4 Data sources for impact evaluation
Data base
Custodian
Data items
Data quality
Data access & issues
ACIR/AIR
Health / DHS
Immunisation records
Concerns about data
Publically available data
quality at 31
Exemption categories, including registered
December 2015 and
Additional data requests to
conscientious objectors and medical exemptions
effect of requirement
be sent to Health
Socio-demographic variables as held in Medicare data
to expand database.
base
No data dictionary as yet
Quality at time of
Geographical data
impact evaluation is
likely to be higher
Child care data
DET
Child care attendance
Quality of data
Privacy issues
dependent on child
Geographical data
care provider records
No formal process for data
being uploaded?
requests
Day one
DHS/Health
CCB and FTB A recipients:
Quality defined as
Ethics and privacy
implementation
•
high due to
considerations to be
reports
Vaccine objectors (based on historical data
requirements for
negotiated with DSS and
prior to 1 January 2016)
accuracy of Centrelink
DHS
• Customers with a grace period
Enterprise data
payment records
•
Warehouse
Immunisation records (current /historical?)
No formal process to
•
(EDW) linked
Payment data for CCB and FTB A
request data
with AIR
supplement
• Reasons for payment withheld
EDW
DHS
Immunisation status data
As above
As above
Socio-demographic data
Geographic data
Social Policy Research Centre 2015
81
link to page 94 link to page 94
In addition, there have been a number of academic studies that have conducted
detailed analysis of ACIR data, including immunisation rates over time
(Beard et al.,
2016).
The advantages of the AIR dataset are that it contains the immunisation records of
all children registered in Medicare or having immunisation records and therefore it is
the broadest population of children. It also contains the data on the different
exemption categories, including conscientious objection up until 1 January 2016.
The disadvantage of the AIR data is that it does not have historical records of
changes in immunisation in individuals, as it is point in time data which is updated
continuously.
The historical aggregate data for immunisation rates could provide baseline data for
assessing the impact of the Measure (changes in immunisation rates). The Health
data could be used in an impact evaluation to:
• analyse and map aggregate changes in immunisation rates across
geographical areas
• link the geographical information to ARIA data to identify changes in
immunisation rates by remoteness
• link the geographical information to SEIFA data to identify the changes in
immunisation rates by socio-demographic status of areas
• identify rates of exemptions, including rates of medical exemptions before
and after the Measure, and rates of Secretary’s exemptions after the
Measure.
Child care data
The data custodian for this data is the DET. Child care service providers provide
information about child care attendance to DET. This data is shared on a weekly
basis with DHS and is merged with data in the EDW to determine eligibility for child
care payments. This data could be used in an impact evaluation to map overall and
geographical patterns in changes in child care attendance before and after the
Measure. However, it would not be possible to determine if the changes in child care
attendance were an outcome of the Measure or due to potential confounding
factors. This may be addressed through qualitative interviews. For example, it may
be possible to undertake case studies in locations where child care attendance has
increased and decreased or where payments have ceased.
Day one implementation reports
DSS advised that the day one implementation reports have been used to monitor
take-up rates and validate issues that might have been included in the risk register.
They were produced by DHS as a result of merging data from ACIR/AIR and EDW.
Based on information provided by the DSS, these reports included the following data
items:
Social Policy Research Centre 2015
82
• All CCB customers and Vaccine Objectors (VO) only records
o Count of customers and children who meet immunisation
requirements by payment types
▪ At least one child meets immunisation requirements
▪ All children are fully immunised
▪ Children have a next immunisation date
▪ Exemption types (natural immunity, medical, vaccine
shortage)
▪ Centrelink override
o Count of Fee Reduction CCB Customers and Children with a Grace
Period applied by payment types
o Count of Fee Reduction CCB Customers and Children with a Grace
Period applied who now meet immunisation requirements
• CCB reduced fee (CCF, CCI, LSC) claims processed
o Granted
o Rejected
o Assessed awaiting ACIR link
o Paid/not paid/Total, pending immunisation or other reason
• FTB-A Immunisation Status Assessed (milestone birthday in the past)
o All children and vaccine objectors (current and expected?)
o Full Payment – DHS FTB Immunisation status
o Full Payment – ACIR FTB Immunisation Status
o No payment
o Link status – yes, not awaiting, mismatch (number of categories)
• Count of CCB Ineligible customers and children due to immunisation non-
compliance (all, All VO)
o CCB Types (CCF LSC, CCF Reduced Fee, CCI, CCR LSC) by
customers that had at least one child ineligible
o CCB Types (CCF LSC, CCF Reduced Fee, CCI, CCR LSC) by count
of all children child ineligible
• Count of Immunisation catch-up letters issued
o Manually issued and auto issued, count of children not immunisation
compliant.
• Reviews and appeals data.
The advantage of these reports is that they provide aggregate data for recipients to
assess the impact of the Measure after the baseline date. These reports are also
produced on a regular basis. The disadvantage of these reports is that they do not
disaggregate data by socio-demographic characteristics of interest or geographic
location in assessing the impact of the Measure.
This data could be used in the impact evaluation to:
• analyse aggregate changes in immunisation rates for CCB and FTB
customers and children by whether they were a vaccine objector or not.
Social Policy Research Centre 2017
83
• analyse the number of CCB recipients who have had payments rejected after
the implementation of the Measure:
o CCB recipients who had a recorded vaccine objection
o CCB recipients who did not have a recorded vaccine objection
• Analyse the number of FTB-A customers who have had part or full
supplements withheld for the 2015–16 tax year, post reconciliation:
o FTB-A customers who had a recorded vaccine objection
o FTB-A customers who did not have a recorded vaccine objection
• Analyse the number of CCB and FTB-A customers who have changed their
status in relating to meeting immunisation requirements (recorded vaccine
objectors and others)
• Analyse the number and outcomes of review and appeals
• Map longitudinal trajectories in key changes in immunisation rates and
impacts on payments for CCB and FTB-A customers by considering changes
in these rates over time prior and after the implementation of the Measure.
DHS Enterprise Data Warehouse
The EDW contains information about child care and FTB payment recipients
necessary to determine payment eligibility. Data items in this data source include:
• socio-demographic variables for children and parents
• child care attendance and eligibility for payment
• geographical residential data
• data on whether immunisation requirements have been met.
The advantages of the DHS data are the more detailed socio-demographic data that
can be linked with child care attendance and payment data, FTB-A data and
immunisation requirement status data. This data is also stored historically for
individuals over time so it is possible to track changes in individual attributes over
time.
If this data is linked with the AIR data, as has been done for the Day One
Implementation reports, a number of analyses would be possible to examine in more
detail the impact on target populations and unintended consequences. The
disadvantage of this data analysis is that it is likely to be time consuming and
therefore more costly to merge and extract the data from both AIR and DHS.
The merged AIR/DHS data could be used in the impact evaluation to:
• extend all day one implementation reports to include a breakdown by key
socio-demographic variables such as:
o parent’s income levels
o parent income support payment type
o family composition
o family size
Social Policy Research Centre 2017
84
o migrant/refugee status of parents
o child’s disability status
o Aboriginal and Torres Strait Islander status
o any record of family violence (if available)
o child protection status (if available)
o housing status
• extend all day one implementation reports to include a breakdown by key
geographical variables linking postcode information with:
o SEIFA indicators to identify impacts on families from low SES areas
o ARIA indicators to identify impacts on families from more remote
areas
• Map longitudinal trajectories in key changes in immunisation rates and
impacts on payments by socio-demographic and geographical
characteristics by analysing changes in rates and loss of payments over time
• Analyse the following changes for CCB and FTB-A payment recipients who
have had a payment rejected/withheld due to not meeting immunisation
requirements by vaccine objector status:
o child care attendance
o employment status of parents
o income levels.
6.4 No Jab, No Pay Impact Evaluation Framework
The aim of the Measure’s impact evaluation will be to measure the impact the policy
has had on immunisation rates at the population level and for particular sectors of
the population, and ultimately to examine changes in the prevalence of vaccine-
preventable diseases. Below we outline options and strategies for impact-related
data collection and analysis. The options and strategies outlined below include
some suggestions that were raised during the stakeholder consultations.
Two key challenges for any impact evaluation relate to isolating the impact of the
Measure on immunisation rates and trying to establish a baseline measure for
determining impact. As noted in the theory of change model above (Figure 2), a
range of additional contextual factors may have had an impact on the immunisation
rates. These include state-based policies, complementary measures introduced by
Health and media coverage of vaccination. As such, isolating the impact of the
Measure on immunisation rates will be a challenge. It may be possible to examine
the impact of outside factors through the qualitative research, which should
complement the administrative data analysis.
An additional challenge relates to the available data in the AIR. The document
review and stakeholder consultation highlighted concerns about the accuracy of the
data in ACIR, now the AIR. It was noted that although some children may have been
immunised, their immunisation records were not up to date. The introduction of the
Measure resulted in significant effort invested in updating immunisation records in
Social Policy Research Centre 2017
85
the database. If there has been an increase in immunisation rates, it is likely that
some of the recorded rate increase will be due to improvements in the complete and
accurate recording of immunisation data rather than actual increases in the
vaccination rate in the population. Therefore it will be important to separate this
increase from actual increases in vaccination as a response to the Measure. An
additional challenge is determining the baseline measure for determining an
improvement in the immunisation rate. This may have to be established through
DHS data rather than the ACIR itself.
6.4.1 Questions:
We begin by outlining a range of questions that could be addressed in any impact
evaluation. These questions encompass the achievement of the Measure’s intended
goals, the extent to which changes can be attributed to the Measure, unintended
impacts, cost-effectiveness and the sustainability of the Measure. The next sections
outline some suggested methods to address these questions and we flag a number
of factors that will influence the design of the evaluation.
1. Did the Measure achieve its intended goal of increasing immunisation
rates and achieving herd immunity in the Australian population?
a. Has there been an increase in immunisation rates since the
Measure?
b. How many previously incompletely immunised children have
engaged in a catch-up schedule?
c. How many children of recorded vaccine objectors have become
immunised since the implementation of the Measure?
d. Have any increases in immunisation rates been sustained over time?
e. How effective were the communication strategies in raising
parents’/vaccination providers’/childcare providers’ awareness of the
policy change?
2. To what extent can changes in immunisation rates be attributed to the
Measure?
a. To what extent are recorded changes due to improvements in data
collection and recording practices, as opposed to real increases in
immunisation rates?
b. What has been the impact of other factors occurring simultaneously
(e.g. state No Jab, No Play policies or other parenting payment
policies)?
c. What was the impact of incentive payments on vaccination
providers?
d. Did the media coverage of the Measure influence behaviour change?
Social Policy Research Centre 2017
86
3. Were there any unintended impacts (positive or negative) of the
Measure?
a. How did the Measure’s impact vary across areas of different socio-
economic status and in different geographic regions?
b. What was the Measure’s impact on families with children born
overseas or recently arrived families?
c. Among parents, is there evidence that disadvantaged groups
experienced:
i. Loss of payments/income?
ii. Reduced child care attendance?
iii. Lower parental employment rates?
4. Is the Measure cost-effective? (cost benefit analysis)
a. How effective is the policy in comparison with alternative
interventions (to be drawn from the literature i.e. whether incentives
are better than sanctions)?
5. Have there been any ongoing implementation challenges following the
post implementation phase?
a. Have all issues, risks and complex scenarios been effectively
addressed?
b. Is the Management Information (AIR/EDW) of sufficient quality to
adequately monitor eligibility for payments and ongoing impacts of
the Measure?
c. Are any impacts likely to be sustained (i.e. will governance structures
remain in place? Impact of phasing out of FTB-part A end of year
supplement – will no longer act as policy lever?)
6.4.2 Suggested methods/design
We recommend that any impact evaluation adopt a ‘before and after’ mixed method
design as it will not be possible to utilise a counterfactual or comparison group to
assess impact.
Quantitative data analysis:
As outlined in the Data Scoping section above, the issues to be explored through
quantitative data analysis of departmental data would include an assessment of the
impact of the Measure on changes in immunisation rates in target populations over
the short, medium and long-term. This analysis would use the data linkage from
DHS and ACIR to extend Day One Implementation reports to include:
Social Policy Research Centre 2017
87
• an analysis of socio-demographic characteristics of customers whose
children meet or do not meet immunisation requirements
• an analysis of geographic location of customers whose children meet or do
not meet immunisation requirements
• analysis of whether the children with a historical register of
conscientious/vaccine objection meet immunisation requirements.
This analysis would require regular detailed reports (quarterly) to be extracted from
the DHS/AIR databases over the period from the baseline date of 1 January 2016
until the end of the impact evaluation assessment period in 2018. DHS would need
to provide data for the impact evaluation researchers (due to privacy considerations)
and as such, DHS would incur costs that would need to be factored into the budget
for the impact evaluation.
2.
Consequences for disadvantaged groups including:
• loss of payments; this analysis would be based on DHS EDW data and
would require data extraction based on the Day One Implementation reports
for categories of disadvantaged groups as outline in the Data Scoping
section above. These would be regular reports to look at changes over time
in groups who have lost payments or become up to date with immunisation
requirements
• lower family income; data on the average amounts of payment lost would
also be required from the DHS EDW for disadvantaged groups
• decline in child care attendance; this data could be sourced from the Child
Care Management system at DET or the DHS data. The analysis would
consider the trends and patterns of child care attendance for children who do
not meet immunisation requirements by socio-demographic characteristics
(DHS) and geographical characteristics (DET or DHS)
• parental workforce participation; analysis of data from DHS for customers in
receipt of income support payments for whom data on employment
status/hours/income and data on children meeting immunisation status is
collected
• increase in the number of medical exemptions (addressing the concern that
COs started applying for medical exemptions after 1 January); this data
could be sourced from ACIR/AIR examine pre and post implementation rates
of medical exemptions.
The analysis for this component of the impact evaluation would rely on data
extracted from DHS EDW and ACIR/AIR over a 2–3 year period and would therefore
incur costs for DHS and Health that would need to be accounted for in the impact
evaluation budget.
Social Policy Research Centre 2017
88
Qualitative data collection:
We recommend that qualitative data collection be undertaken with a range of
stakeholders to gain their views on the impact of the Measure. The qualitative data
will explore evaluation questions 2, 3 and 5 (and their sub-questions): the extent to
which changes can be attributed to the Measure, unintended impacts and the
sustainability of the Measure’s impact.
We recommend that qualitative data collection be conducted in multiple sites in
NSW, Queensland and Victoria as these three states also have
No Jab No Play policies. We also recommend including one other state. The qualitative data
collection should be conducted in urban, regional and remote sites. The qualitative
data collection could include both one-to-one in-depth interviews (face-to-face and
by phone) and focus groups where possible. One option would be to conduct case
studies in particular geographic locations, which could be chosen according to a
range of criteria including:
• above/below average increases in vaccination rates
• rates of cancelled child care payments and/or FTB-A supplement
• low baseline vaccination rates/high conscientious objection rates
• other criteria (e.g. appeals, Secretary’s Exemptions etc.).
Stakeholder groups:
1. policy staff; as the Measure was introduced by the Australian Government,
with on the ground implementation at state level, any impact evaluation
should consult with policy staff in at both levels of government in the four
nominated states.
2. general practitioners & vaccination providers; any impact evaluation should
include consultation with general practitioners and vaccination providers in
the four states. This consultation will help identify the impact of incentives,
whether vaccine confidence has increased, barriers to and facilitators of
immunisation and any issues with recording and updating immunisation data
(including incomplete records, software issues, any increase in requests for
medical exemptions since the introduction of the Measure).
3. parents; consultation with a range of parents directly affected by the
Measure is critical for assessing the impact of the Measure on changing
behavior. Consultation should be undertaken in all four states and a stratified
sampling approach used to ensure that the following groups of parents are
selected for consultation:
•
parents who choose to vaccinate
•
those who vaccinate because they feel compelled to (who may have
otherwise have lodged a conscientious objection)
•
those who choose not to vaccinate
Social Policy Research Centre 2017
89
link to page 76
•
parents of incompletely immunised but not vaccination objectors
•
parents of children vaccinated overseas
•
parents seeking medical exemptions
Consultation with parents should explore their perspectives on immunisation
in general (health benefits vs fear of losing payments, vaccine confidence,
barriers and enablers to vaccination), their child’s immunisation status,
whether the Measure prompted any change in their child’s immunisation
status, whether they incurred a financial loss as a result of the Measure or
whether their child care or workforce participation changed following the
introduction of the Measure. It should be noted that accessing parents,
especially those who are vaccine hesitant or objectors, will be challenging.
Recruitment may have to be done through a number of different methods
including social media, service providers, Centrelink etc.
4. experts; An additional group of stakeholders that might be included in any
impact evaluation are experts in public health and immunisation. Ideally,
these stakeholders would have a good understanding of the ACIR/AIR and
the relative impact of using payments as a lever versus the impact of
accompanying support (e.g. communications with doctors) to encourage
behavioural change.
Economic evaluation
The economic evaluation could draw upon the findings of any impact evaluation and
will model the economic costs and benefits of vaccinating additional children after
the onset of the Measure. Where possible, this analysis will include a geographical
breakdown, as the benefits of vaccinating a child living in an area with low
vaccination rates will be greater than a child living in an area with already high rates
of vaccination. Similarly, if possible, the modelling will include vulnerable groups
such as Aboriginal and Torres Strait Islander and CALD children who are at higher
risk of vaccine preventable disease.
The analysis should include the Australian Government and state and territory costs
of implementing the Measure as well as direct savings from the FTB supplement and
CCB components of the Measure. Where possible, the analysis should also include
the costs and benefits of unintended consequences of the Measure (e.g. reduced
parental workforce participation, reductions in child care uptake) indicated in section
6.2.1.
6.4.3 Evaluation timescales
The design could include staged data collection/analysis – to determine short,
medium and long-term impact.
One stakeholder felt that any impact evaluation should commence sooner rather
than later as stakeholders’ recollections will fade if it is delayed. However, because
Social Policy Research Centre 2017
90
of the way FTB is calculated, the improvements to the AIR due in 2017 and the
availability of data the most appropriate timescale for the evaluation would be mid-
2017–mid-2020.
6.4.4 Costs of evaluation
A broad estimate of the costs of the evaluation would be around $400 000. This
would include analysis of administrative data including data linkage with a number of
datasets, qualitative interviews with stakeholders and five geographical case studies
in different communities. These costs would be reduced if:
• some of the data linkage and/or analysis was conducted internally by
DSS/DHS
• fieldwork did not involve interviews with parents
• case studies were reduced to three geographical areas.
Social Policy Research Centre 2017
91
7 References
Abbott, T. (2015).
Joint Doorstop Interview, Sydney, PM Transcripts, Transcripts
from the Prime Minister of Australia. Online:
http://pmtranscripts.pmc.gov.au/release/transcript-24358.
Adams, J., McNaughton RJ, Wigham S, Flynn D, Ternent L, & J, S. (2016).
Acceptability of Parental Financial Incentives and Quasi-Mandatory
Interventions for Preschool Vaccinations: Triangulation of Findings from
Three Linked Studies.
PLoS One, 11(16), : e0156843.
doi:0156810.0151371/journal.pone.0156843.
Australian Government. (2014).
National Immunisation Strategy for Australia 2013-
2018. Department of Health, Commonwealth of Australia.
Australian Government. (2015a).
Detailed Requirements Document (DRD)
Supplementary Requirements Document, EXTENDING IMMUNISATION
REQUIREMENTS – CATCH-UP ARRANGEMENTS FOR >10 YEAR OLDS.
Costing Reference: 002521, Version: 0.3. Canberra: Australian
Government.
Family Assistance (Meeting the Immunisation Requirements) Principles 2015, A
New Tax System (Family Assistance) Act 1999 (2015b).
Australian Government. (2015c).
Improving Immunisation Coverage: General
Practitioners and Vaccination Providers - Communication Activities.
Australian Government. (2016a).
ACIR - Annual Coverage Historical Data,
Immunise Australia Program. Online.
Australian Government. (2016b).
Family Assistance Guide Version 1.190 - Released
7 November 2016. Online: http://guides.dss.gov.au/family-assistance-guide.
Australian Government. (2016c).
National Immunisation Program Schedule, From
November 2016. Online: Retrieved from
http://www.immunise.health.gov.au/internet/immunise/publishing.nsf/Content
/5403D77C07E1973ACA257D49001E3775/$File/NIP-schedule2016.pdf.
Australian Government. (no date).
UPDATE: No Jab No Pay – Immunisation Catch-
Up Arrangements.
Australian Goverrment. (2015).
No Jab, No Pay – New Immunisation Requirements
for Family Assistance Payments.
Beard, F., Hull, B., P., Leask, J., Dey, A., & McIntyre, P. B. (2016). Trends and
patterns in vaccination objection, Australia, 2002e2013.
Medical Journal of
Australia, 7(-), -.
Communication and Media Branch. (2015).
Extending Immunisation Requirements
(No Jab, No Pay) Communication strategy.
Constable, C., Blank, N. R., & Caplan, A. L. (2014). Rising rates of vaccine
exemptions: Problems with current policy and more promising remedies.
Vaccine, 32(-), 1793-1797.
Danchin, M., & Nolan, T. (2014). A positive approach to parents with concerns about
vaccination for the family physician’.
Australian Family Physician, 43(10),
690-694.
Department of Health. (2016). Immunise Australia Program, Immunisation Coverage
Targets. Retrieved 21/02/2017
Department of Social Services. (2016).
Evaluation Background Summary – No Jab,
No Pay. Australian Government Department of Social Services,.
Dube, E., Gagnon, D., MacDonald, N., E., & The SAGE Working group on Vaccine
Hesitancy. (2015). Strategies intended to address vaccine hesitancy: Review
of published reviews.
Vaccine, 33(-), 4191-4203.
Social Policy Research Centre 2017
92
Dubé, E., Gagnon, D., Ouakki, M., Bettinger, J., Guay, M., Halperin, S., . . .
MacDougall. (2016). Understanding Vaccine Hesitancy in Canada: Results
of a Consultation Study by the
Canadian Immunization Research Network,.
PLoS One 11(16).
Forbes, T. A., McMinn, A., Crawford, N., Leask, J., & Danchin, M. (2015).
Vaccination uptake by vaccine-hesitant parents attending a specialist
immunization clinic in Australia.
Human Vaccines & Immunotherapeutics,
11(12), 2895-2903.
Gibbs, R. A., Hoskins, C., & Effler, P. V. (2015). Children with no vaccinations
recorded on the Australian Childhood Immunisation Register.
Australian and
New Zealand Journal of Public Health, 39(3), 294-295.
Harvey, H., Reissland, N., & Mason, J. (2015). Parental reminder, recall and
educational interventions to improve early childhood immunisation uptake: A
systematic review and meta-analysis.
Vaccine, 33(-), 2862-2880.
Hull, B., Dey, A., Beard, F., Menzies, Brotherton, J., & McIntyre, P. (2013).
Immunisation coverage annual report, 2013.
Communicable diseases
intelligence quarterly report, 37(1), 21-39.
Jacob, V., Chattopadhyay, S. K., Hopkins, D. P., Murphy Morgan, J., Pitan, A. A.,
Clymer, J. M., & the Community Preventive Services Task Force. (2016).
Increasing coverage of appropriate vaccinations: A community guide
systematic economic review.
American Journal of Preventive Medicine,
50(6), 797-808.
Jarret, C., Wilson, R., O’Leary, M., Eckersberger, E., & Larson, H. (2015). Strategies
for addressing vaccine hesitancy – A systematic review.
Vaccine, 33(34),
4180-4190.
Lawrence, G., MacIntyre, C., Hull, B., & McIntyre , P. (2004). Effectiveness of the
linkage of child care and maternity payments to childhood immunisation.
Vaccine, 22(17-18), 2345-2350.
Leask, J. (2015). Should we do battle with antivaccination activists?
Public Health
Research & Practice, 25(2), 1-4.
Leask, J., & Kinnersley, P. (2016). Physician Communication With Vaccine-Hesitant
Parents: The Start, Not the End, of the Story.
Pediatrics, 136(1), 180-182.
Leask, J., Kinnersley, P., Jackson, C., Cheater, F., Bedford, H., & Rowles, G.
(2012). Communicating with parents about vaccination: a framework for
health professionals.
BMC Pediatrics, 12(-), 154-165.
Leask, J., & Wiley, K. (2015). Submission 327 to Inquiry into the Social Services
Legislation Amendment (No Jab, No Pay) Bill 2015.
Leask, J., Willaby, H. W., & Kaufman, J. (2014). The big picture in addressing
vaccine hesitancy.
Human Vaccines & Immunotherapeutics, 10(9), 2600-
2602.
Macartney, K. (2015). Forget ‘no jab, no pay’ schemes, there are better ways to
boost vaccination.
Australian Medicine, the Australian Medical Association,
27(3), 21-22.
Mantzari, E., Vogt, F., Marteau, T., & Kazak, A. (2015). Financial Incentives for
Increasing Uptake of HPV Vaccinations: A Randomized Controlled Trial.
Health Psychology, 34(2), 160-171.
National Centre for Immunisation Research & Surveillance. (2016). No Jab No Play,
No Jab No Pay Policies. Retrieved 18/10/16, 2016
Parliament of Australia. (1999). A New Tax System (Family Assistance) Act 1999,
No. 80, 1999.
Social Services Legislation Amendment (No Jab, No Pay) Act 2015, No. 158, 2015.
An Act to amend the law relating to family assistance, and for related
purposes. (2015).
Social Policy Research Centre 2017
93
Budget Savings (Omnibus) Act 2016, No 55, 2016 (2016).
Patton, M. Q. (1990).
Qualitative Evaluation and Research Methods (2nd ed.).
Newbury Park, London, New Dehli: Sage.
Pearce, A., Marshall, H., Bedford, H., & Lynch, J. (2015). Barriers to childhood
immunisation: Findings from the Longitudinal Study of Australian Children.
Vaccine, 33(-), 3377-3383.
Porter, C. T. H. (2015). 2UE Interview with Justin Smith, 23 November 2015.
Porter, C. T. H. (2016a).
No Jab, No Pay lifts immunisation rates. Canberra.
Porter, C. T. H. (2016b).
Tasmania leads childhood immunisation rate improvement
as Indigenous immunisation rates soar. Canberra: Australian Government.
Public Health Association of Australia. (2015). Submission 317 to Inquiry into the
Social Services Legislation Amendment (No Jab, No Pay) Bill 2015.
Rollins, A. (2015). Govt banks on massive savings from No Jab No Pay policy.
Australian Medicine, Budget Edition 14 May 2015(-), 16.
Salmon, D., Teret, S., MacIntyre, C., Salisbury, D., Burgess, M., & Halsey, N.
(2006). Compulsory vaccination and conscientious or philosophical
exemptions: past, present, and future.
Lancet, 367(9508), 436-442.
Senate Community Affairs Legislation Committee. (2015).
Report of the Senate
Community Affairs Legislation Committee on Social Services Legislation
Amendment (No Jab No Pay) Bill 2015. Canberra: Commonwealth of
Australia.
The Hon Sussan Ley MP. (2015).
$26m booster to Immunise Australia.
http://www.health.gov.au/internet/ministers/publishing.nsf/Content/health-
mediarel-yr2015-ley044.htm.
The Royal Australasian College of Physicians. (2015). Submission to Inquiry into the
Social Services Legislation Amendment (No Jab, No Pay) Bill 2015.
Victorian Government. (2016). Frequently asked questions: No Jab, No Play.
Retrieved 27/10/16, 2016, from
https://www.betterhealth.vic.gov.au/campaigns/no-jab-no-play
Ward, K., Chow, M. Y. K., King, C., & Leask, J. (2012). Strategies to improve
vaccination uptake in Australia, a systematic review of types and
effectiveness.
Australian and New Zealand Journal of Public Health, 36(4),
370-377.
Ward, K., Hull, B. P., & Leask, J. (2013). Financial incentives for childhood
immunisation — a unique but changing Australian initiative.
Medical Journal
of Australia, 168(11), 590-592.
Wigham, S., Ternent, L., Bryant, A., Robalino, S., Sniehotta, F., & Adams, J. (2014).
Parental Financial Incentives for Increasing Preschool Vaccination Uptake:
Systematic Review’.
Pediatrics, 134(4), 1117 – 1128.
Williams, S. E. (2014). What are the factors that contribute to parental vaccine-
hesitancy and what can we do about it?
Human Vaccines &
Immunotherapeutics, 10(9), 2584-2596.
World Health Organization. (2013). Global Vaccine Action Plan 2011-2020. Geneva:
World Health Organization.
Social Policy Research Centre 2017
94